Series
The Location of Justice
An examination of the pervasive and often overlooked infrastructure of criminal justice in New York and the spaces that could serve a more just city.
In This SeriesWe are celebrating 15 years — and counting — of stories that are deeply researched and deeply felt, that build a historical record of what the city has been.
The average jail or prison bears little resemblance to a therapist’s office, a community mental health clinic, an inpatient psychiatric facility, or any other therapeutic environment. Indeed, the restrictive and often chaotic jail or prison environment can exacerbate or even cause mental health problems for people inside. The use of solitary confinement is only the most extreme example. So how does a criminal justice system organized around security and punishment provide therapeutic care? Could there ever be room for privacy, tranquility, or other preconditions of emotional growth? As national problems of mental health care and criminal justice become more and more interwoven, these are not hypothetical questions.
People with mental illness are arrested in large numbers, and once in custody they stay there longer, given they are less likely than other people to be bailed out, to get good plea deals, or to be given alternatives to incarceration. So while the number of incarcerated people has begun to decline in recent years, the proportion diagnosed with some form of mental illness has been going up. The result, as Alisa Roth details in her recent book, Insane: America’s Criminal Treatment of Mental Illness, is that correctional facilities have become some of the largest de facto mental health providers in the country. New York City is no exception. In 2014, almost 40 percent of the population on Rikers Island had some diagnosis of mental illness (meaning they received treatment at some point during their stay). While in 2015 the NYPD estimated that it responded to 12,000 mental health calls per month. When a city addresses mental health crises through law enforcement, the consequences can be tragic. In April, Saheed Vasell, a Crown Heights resident diagnosed with bipolar disorder, was shot and killed by police, one of ten mentally ill people killed by NYPD in the last three years. Abuses in solitary confinement units for mentally ill detainees on Rikers Island led to the deaths of two men in 2013 and 2014, amid broader reports of high rates of physical violence against the jail’s population with mental illness. More recently, the city has proposed a series of changes to the treatment of mentally ill people in the criminal justice system and at Rikers, with new policies ending “punitive segregation” for detainees with serious mental illness, as well as juveniles under the age of 21, and new intensive care housing units for patients with serious mental health issues. In 2016, NYC Health and Hospitals, the largest public health care system in the country, took direct control of the care of people in the city jail system (it was previously administered by Corizon, the largest for-profit private contractor of medical services to jails and prisons in the country).
Today, NYC Health and Hospitals operates one of the nation’s largest correctional health care services, including providing comprehensive mental health care to people in the criminal justice system from before they are arraigned to after their release from detention. NYC Health and Hospitals also administers inpatient psychiatric services at Bellevue and Elmhurst Hospitals and four borough court clinics. Dr. Elizabeth Ford is NYC Health and Hospitals’ Chief of Psychiatry for Correctional Health Services (CHS). She spent 15 years working in Bellevue Hospital’s inpatient psychiatric unit for men held at Rikers Island, beginning as a psychiatric intern and becoming director of the program. In 2014, satisfied with the changes to patient care implemented at the hospital, and concerned with the state of care in the jails themselves, Dr. Ford went to work at Rikers. From her office there, where the window is reinforced with double barbed wire and the sound of planes taking off from La Guardia Airport regularly intervenes, she talked to UO. Ford spoke about the challenges of treating mental health patients in a punitive environment, to the changes CHS has been bringing to spaces of confinement and treatment on Rikers Island, and the kind of mental health system that could serve New Yorkers better, both in and out of the criminal justice system.
I see my role as trying to help the jail be as therapeutic a place as possible. I don’t think jails are the space where people should be getting their mental health care, but for those who are in jail, we should do the very best that we can for them.
We have a mental health staff of around 500 people, from about 15 different disciplines, and we work very closely with the Department of Corrections (DOC). The overall jail population is around 9,000 and it’s going down. Of the people who are here, about 40 percent are either currently receiving mental health treatment or have at some point in their stay with us. Of that 40 percent, about a quarter have what’s called serious mental illness: For us, that means schizophrenia, bipolar disorder, major depressive disorder, or post-traumatic stress disorder. So that’s roughly eleven to twelve percent of the total jail population.
I’m not sure I thought I would say this when I started this job, but I’m very proud of what the jail system is able to offer. When someone gets admitted to the jail, they get a medical workup, lots of primary care interventions. At that point a referral can be made to the mental health service based on concerns from the patient or the doctor, or if they’ve had treatment in the community. And then we, the Mental Health Service, will see people within three days, and assess the severity of their illness and the level of intervention that they need. If, when they first come in the jail, they’re not referred to mental health, they can be referred at any time during their jail stay. We have a really robust referral system. Attorneys, family members, sometimes judges; the DOC refers a ton of patients to us.
The majority of the patients we see go into general population housing (GP), where they live with everyone else in the jail and come to a clinic to get healthcare. In GP, they’ll see a psychiatrist at least every month and a therapist at least every couple of weeks. We don’t have any control over the GP housing areas; they differ based on when the jail was built and the architecture, but you generally will have either a dorm setting or individual cells. There are 35 to 50 single-level beds per dorm, lined up next to each other, with a little space for personal belongings.
In cell housing, which is the alternative, there’s one person per cell, and people have to ask permission and get somebody’s attention to get in and out of their cells. Unless they happen to be in punitive segregation, they’re not locked in the cell unless there’s an acute safety issue. But generally people have their own space. Sometimes the cell houses are very dark, like a corridor with cells off the side; sometimes they’re bright and airy.
There are patients who do better or worse in each of those settings. Dorms tend to not be great for all people — forget mental illness — who don’t want to be around a lot of other people that they’ve never met or whom they are afraid of, or for people who tend to be aggressive. Dorms are better for people who we may be concerned about hurting themselves, largely because of all those extra eyes on someone. There’s less space to hide.
Mental Observation (MO) houses are residential housing units for people, largely with serious mental illness, but also those who are particularly vulnerable for some reason in the GP setting. Currently 18 of those are peppered throughout seven of the jails. These are protected spaces, where the staff take care of the patients in the units. A team, led by a psychologist but also including a psychiatric provider, a social worker, an arts therapist, and sometimes a substance abuse counselor, will all take care of the same group of patients.
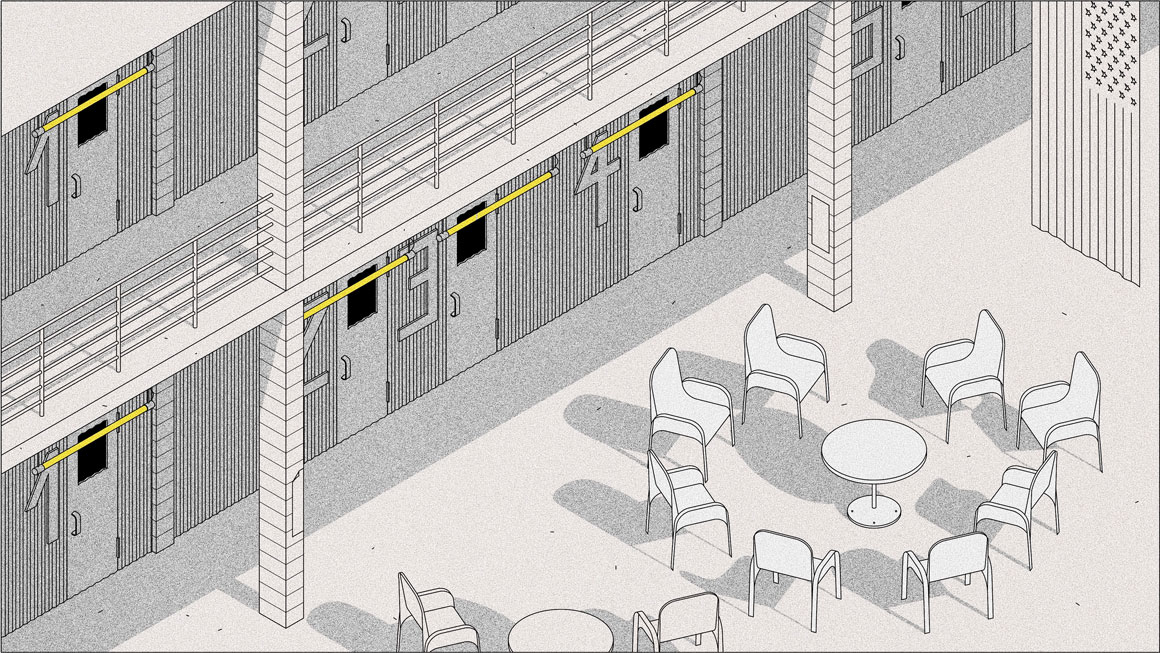
What distinguishes MO units, physically, from general population units is interview space. There’s a space somewhere in that unit where a clinical staff member can have an, as confidential as possible, interview with somebody. As you can imagine, it would be very difficult to go to someone’s cell door, and through the little food slot, have a therapy session. Sometimes, unfortunately, that’s the best we can do, but on the MOs there’s designated space for these sessions to happen. Sometimes it’s formally set aside, but otherwise we just have chairs in a circle so there’s space for group therapy to happen.
Mental Health had more input into the design of those units. These are cohorts of people with serious mental health needs and we wanted to be thoughtful about that space for them. I think we should be thoughtful about the space for everybody’s needs here, and frankly everybody who works here. Do people with mental illness have different environmental needs? Largely, no. People who are detained in a space, without autonomy, with rules that sometimes they don’t understand or that are not consistently followed, with people coming in and out at a rapid pace — that kind of stuff affects everybody here, whether they have mental illness or not. If you provide an environment where people can thrive, even in a jail — I know that sounds a little strange — they will grow. People will rise to your expectations, in my experience. And if you put them in a space where they’re shut down and confined, and you expect that they’re going to behave badly, then they will do that. It’s very fear-based. I think the more that jails and prisons can inspire human beings to be thoughtful, the more rehabilitated they can become, and the better for that. At least with the mental health population, we’ve been trying our best to do some of that.
We had a lot of input into the design of the PACE (Program to Accelerate Clinical Effectiveness) units, the highest level of care in the jail. On those six units, we were as thoughtful as we could be about the architecture. All but one unit are cell houses. We wanted to have a lot of open space. They have as much light as possible given the facility. Some of our patients are in a very old facility, and the light is admittedly not great, but we tried to choose a paint color that would hopefully brighten things up. Two PACE units are in a newer jail that is right across from LaGuardia with giant windows and this giant atrium, and that feels therapeutic in some way. There’s space for people to walk around and look outside. We wanted to have a separate interview room, to actually have a space where you could close the door or mostly close the door so that what we discuss in the group is as confidential as possible. We wanted to have a lot more interview rooms, and offices on the unit so that staff are available to the patients as much as they need them.
Once these units open, they give a peek into what works in this environment. For example, in one of the units they painted chalkboard paint on the cell doors so that messages could be written to the patients if they were asleep or so that their name could be on the door to try to create a community feel. Or turning what used to be a cell for an individual into a quiet space where anyone can go and get away from things, just to take a few breaths and try to be mindful. We also have a nursing office, so patients no longer have to disrupt all of the things that are happening for them in the unit in order to leave and go to the clinic.
Things like confidentiality come up very frequently in the discussion about PACE units. From a mental health perspective, as long as it’s not putting ourselves or the patient in danger, we want a space where no one can hear what we’re talking about with the patient. There’s a lot of stuff that can be very sensitive, things that we don’t want fellow patients and definitely not officers or sometimes even other staff to hear. But from DOC’s viewpoint, if you’re in a locked room by yourself with someone and people can’t get in, that’s a real security problem. So the compromise in some units has been rooms that have huge visibility panels and have locking mechanisms where you can get easily in and out but still close the door, and officers who are standing outside of the room can see everything’s that going on but can’t hear it.
When we have some patients who are locked in their cells for whatever reason, and DOC thinks that it’s too risky for them to come out to talk, that is a very difficult dynamic. The risk-benefit analysis is whether to go to someone’s cell door and try to have a conversation with them while an officer is standing right there, hearing everything, or to not have a conversation at all with that patient. There’s an expectation that if you can’t offer complete confidentiality and privacy in mental health care, you’re failing the patient. And I think that absolutist approach, frankly, is a little ill-informed. It’s not in line with the environment. We are very focused on harm reduction. We are trying to do the very best we can, given the givens.
The balance between what is therapeutic and what is secure is really the art of this work. But the relationship with DOC has improved considerably, to the point where there are sometimes officers that are suggesting changes that are more therapeutic than what we’re suggesting.
For instance, one of the units has two tiers. From a mental health perspective a balcony without any protection is very dangerous. People could jump off it, and have in the past. The officers all agreed about that, and then the discussion was, what sort of barrier do we put up there? Should we do chain link fence? Should we do plexiglass? Or should we do this horizontal bar stock? The DOC pointed out that the plexiglass wouldn’t look like so much of a barrier, but the ventilation would be so bad that it would be super hot in those cells and people would be very uncomfortable. That’s not good for the patient. And then the chain link doesn’t prevent things like hanging. We settled on the horizontal bar stock, and nobody was super happy with that just because it looked more jail-ish, but one officer suggested painting it a different color. It helped a ton. And it’s the least loopable and the most air quality-friendly, and no one has injured themselves on those bars since that unit opened.
Since the introduction of the PACE units, and on the MOs, where there wasn’t a whole lot of environmental work done but where things have shifted over time in terms of the culture, we now have greatly reduced incidents of self-injury and violence; we don’t hospitalize people anywhere near the rates we used to. And on the PACE units, particularly, the patients are much more engaged in their treatment than we’ve ever seen. So the model, we think, is definitely working. And at the jail level, we haven’t had a suicide in over two years. Suicide is the single leading cause of death in jails in this country, not just among people with mental illness. I do think it speaks to a collective approach to caring for people with mental illness and to caring generally for people in the jail.
At Rikers, there is a population that is sentenced and stable, in the sense that they come in and they know when they’re getting released. Those individuals are for the most part all in the same jail, which functions a lot more like a prison in the sense that individuals there can be involved in programs that last a long time. Someone could be, for example, in a twelve-week cognitive behavioral therapy program, because the staff and the patient both know they’re not leaving until a given date.
For the 85 percent of the jail who are not sentenced, it’s extremely difficult to plan continuity of care and reentry and think about connecting someone back into the community, because we don’t know when they’re going back. Not being able to have control of the discharge is really difficult for a mental health provider, because that’s a very important end to a relationship and can often take months.
We are assuming two things about our patients: one, that they’re going to be with us for a long time, and two, that they’re leaving tomorrow. We start thinking about reentry planning and medications and contacting family and community providers as soon as possible. But then we also spend however much time we have with that individual trying to figure out the right diagnosis, creating treatment plans that may take months, but that we’ll try to start. We try as best we can to keep the patients prepared for an abrupt relationship end and also try to foster a strong relationship at the same time. It can be very jarring.
I think we need a system of care where there are fewer boundaries between providers and patients. The model in my head involves a care provider who takes care of their patient wherever they are in jail, or in a hospital, or in a community clinic, or working their way through the court, or in a shelter, any place. These patients track through so many different levels of care, administered by lots of different agencies. It’s very hard to have the kind of communication amongst those agencies that I think is necessary to help these people maintain stability and live in the community.
We’re pretty good at taking care of people who are really sick and who need to be in a hospital. And we’re pretty good at taking care of people who are functioning fairly well in the community, who come to their appointments and basically just need a little bit of support. But we are not great at the large population of people who fall in between. When they come to the jail, we’re much better at it. But still, [if you’re a provider of care in the community] your patient goes to jail and then you lose them, and then they come back out, and oh, here they are again. That’s not a good model of care in general and particularly for people with mental health issues.
Care should be blind to whether the patient is arrested or not. A lot of community providers don’t want to take care of people who are incarcerated. It comes with this stigma that people who are in jail are this different, scarier group of people than everyone else, and that’s just not true.
The views expressed here are those of the authors only and do not reflect the position of The Architectural League of New York.
An examination of the pervasive and often overlooked infrastructure of criminal justice in New York and the spaces that could serve a more just city.
In This Series