



Series
Well-Placed
In the face of exclusion and displacement, how do communities mobilize urban space for mental health and collective wellbeing?
We are celebrating 15 years — and counting — of stories that are deeply researched and deeply felt, that build a historical record of what the city has been.
In trying times (take a look around), New York City, at its best, offers a sense of belonging to buffer against the proverbial storm. Whether found in official policies and resources, or in the open arms of communities large or small, sanctuary can be just as much a state of mind as it is a physical place and social compact. Benefiting from inclusive and collective forms of citymaking on one hand, and facing displacement and disregard on the other, New Yorkers may not necessarily all be “in this together,” but they’re not necessarily on their own, either. To chart this uneven geography of mental health — traversing mind and urban matter — we’re partnering on a new special series as part of Mindscapes, an international cultural program that aims to support a transformation in how we understand and address wellbeing. Well-Placed will focus on people for whom the city does not already work well, and how they mobilize to create spaces that foster both collective power and greater peace of mind: from the city’s Arab diaspora taking to the streets in solidarity with protestors in Lebanon, Syria, and Palestine; to designers working to install a rare, fully-accessible piece of play equipment; to queer youth seeking sanctuary and fun at the New York Public Library’s anti-Prom.
Below, Jessica Fletcher and Helena Najm start us off by taking a look at Harlem’s long-shuttered Lafargue Clinic, a pioneering space that provided mental health treatment for people experiencing racial discrimination. Established in 1946 through the unlikely partnership of a German-Jewish immigrant psychiatrist and a giant of 20th-century American literature, the clinic set up shop in the basement of a parish house, attached to a local church designed by New York State’s first registered Black architect. Over the course of the next decade, the clinic’s unusual focus on dignified, context-specific healthcare for its neighbors would make humble, but significant ripples across the city, state, and country beyond — its influence still felt today in efforts to make “the good life,” and good feelings, accessible to all.
“Clinic for Sick Minds: Basement of a Harlem Church is Haven for the Mentally Ill” ran the headline in a February 1948 issue of LIFE magazine article documenting the Lafargue Clinic. Tucked between pages showing the rags to riches story of the new Mrs. Winthrop Rockefeller, a luxurious skiing season at an Oregon resort in 15 pages of color, and the Westminster Kennel Club pedigree dog show, were photographs of a young Black veteran receiving mental health care, a Black mother and child consulting with a doctor, and a white housewife seeking aid with her criminal trial after shooting her abusive husband. The article emphasized the clinic’s egalitarian nature, noting that it had been founded by the German psychiatrist Frederic Wertham, who believed “that expert mental health care should be available to all men and not confined to the few who can afford to pay.” Thus rates were set purposefully low: patients paid only 25 cents per visit (around three dollars today), or were seen for free. Known beyond its neighborhood through coverage in national and local media throughout the 1940s, the clinic subsequently faded into obscurity. More recently, scholars have rediscovered its vital importance in the development of anti-racist psychiatry and in understanding how the experience of racial segregation and discrimination affects the psyche.
The Lafargue Clinic opened in March 1946 in the basement of the St Philip’s Church Parish House, located on 133rd Street between Seventh and Eighth Avenues (now Adam Clayton Powell Jr. Boulevard and Frederick Douglass Boulevard, respectively) with a mission of serving the local majority Black and low-income population, who had little access to mental health services. Founded by Wertham and the famed novelist Richard Wright, the clinic sought to address the widespread mental health needs of Harlemites. Crucially, the clinic’s multi-racial staff understood racial discrimination to be a major contributing factor in Harlemites’ mental distress. This was a rare approach. At the time, mainstream psychiatry alternately suggested that Black people were too “primitive” to experience neuroses, or excessively pathologized Black people’s mental health issues, leading to the overdiagnosis of mood disorders (primarily schizophrenia) and the disproportionate representation of African Americans in the city’s psychiatric wards.
Wertham was intimately familiar with this unjust system, having worked at Johns Hopkins Hospital in Baltimore and Bellevue and Queens General Hospitals in New York. His experience in these two deeply segregated cities brought Black people’s subjection to residential segregation, education and employment discrimination, and police brutality into sharp perspective. Born in Nuremberg to a secular Jewish family, Wertham left Germany for the United States after becoming disenchanted with what he saw as a conservative nationalist turn in German psychiatry following World War One. Once in New York in the 1930s, he struck up a friendship with Wright who was living in Harlem, editing The Daily Worker, and advocating for Black Americans.
As the scholar Gabriel Mendes highlights in his book-length study of the clinic, Under the Strain of Color, Wright saw the urgent need for reform in the psychiatric establishment in part because of his own experience with medical professionals. When he was drafted to the US Army in January 1944, he wrote a letter protesting the fact that he was forced to serve in racially segregated armed forces. In response, the draft board categorized him as unfit for service due to severe psychoneurosis, and referred him for psychiatric investigation. Wright himself experienced how officials used psychiatry to pathologize Black men and naturalize racial inequality. Ralph Ellison eventually connected Wertham and Wright to Reverend Shelton Hale, Bishop of St. Philip’s Episcopal Church. Upon learning of their desire to create a mental health clinic in underserved Harlem, he offered to host it in the Parish House basement.
The Church and its Parish House were familiar places to neighborhood residents, and functioned both as spaces of worship and welfare. During the Great Depression, Bishop led the Harlem Cooperating Committee on Relief and Unemployment, a local counterpart to the Mayor’s Official Committee for the Relief of Unemployed, and used contributions from working Harlemites to meet community needs.[1] Bishop had also made great efforts to expand the church’s base from more affluent Black Episcopalians to include working-class migrants from the West Indies and the American South. The clinic joined many other welfare services offered by St. Philip’s Church, including a home for the aged in the row house next door, and formed a local landscape of care for Black New Yorkers.
In his 1948 essay, “Harlem is Nowhere,” Ralph Ellison emphasized the psychological connection between Harlem, its physical location, and the community that emerged from residents’ shared histories of alienation in the United States. In Black Harlemites’ “search for answers to the questions Who am I, What am I, Why am I, and Where?,” the denial of their existence and place in a society that persistently discriminates against them effectively made them “displaced [people] of American democracy.”[2] As Gabriel Mendes has observed, Wertham also used the language of displacement to describe how his patients’ mental health concerns stemmed from the exclusionary environment that they found themselves in when they sought treatment. Black Americans’ migration from the Jim Crow South to the segregated North was a process of uprooting that engendered “loss, dispossession, and instability,” which Wertham likened to the condition of displaced people during World War Two who had no home country to which they could return. When Ellison and Wertham built this framework to explain how the anxiety of surviving in a context of social and physical displacement inhibited Black Americans’ wellbeing and mental health, they formed the basis upon which the congregation of patients in the Lafargue Clinic could create community out of social psychotherapy.
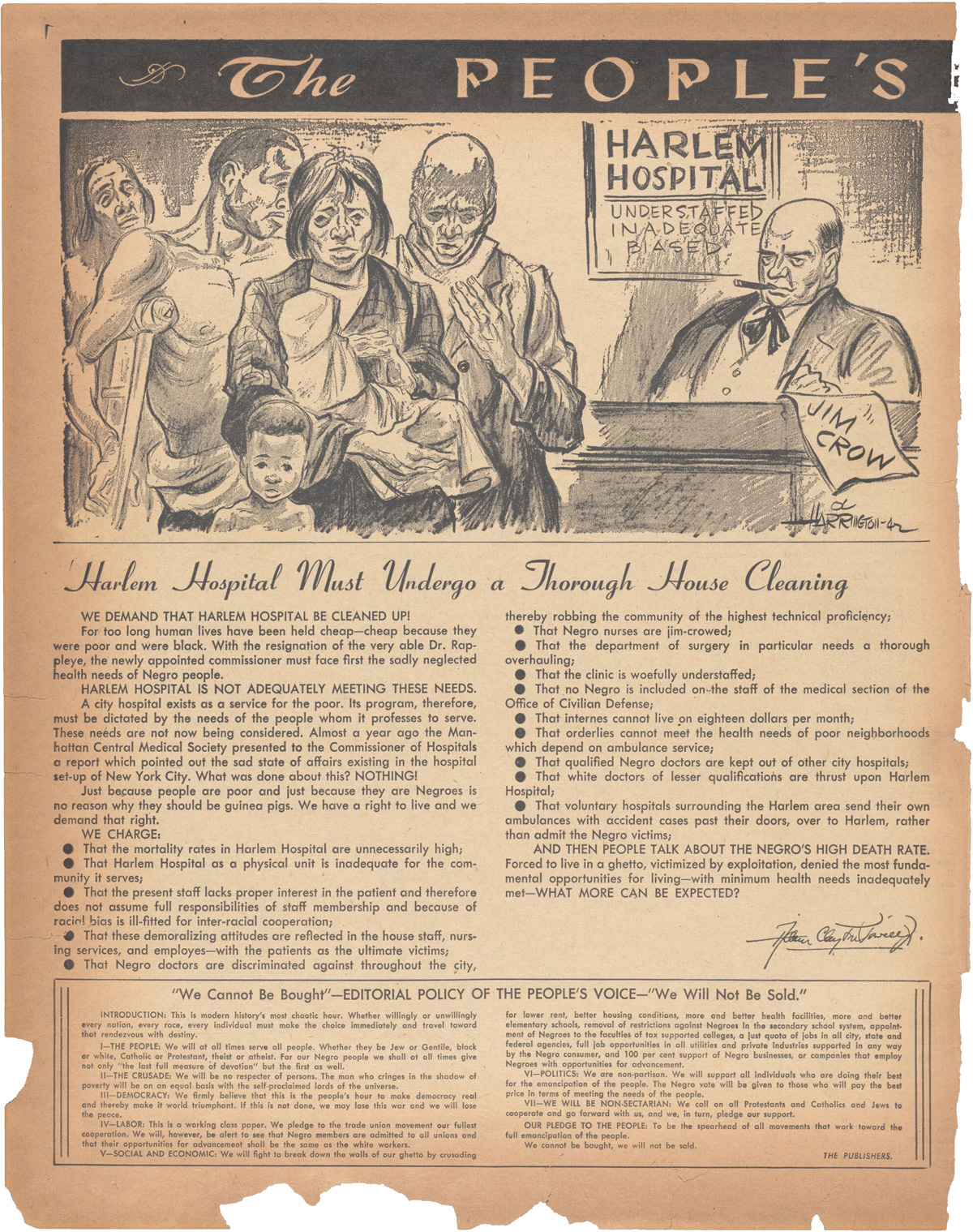
Locating the clinic in the St. Philip’s Church Parish House built upon existing networks of trust and care within the Black community. In an interview with Mendes about her memories of the clinic, Bishop’s daughter, Dr. Elizabeth Bishop Davis Trussell, noted that numerous Harlemites were extremely reluctant to visit mental health clinics run by the city. When her father advised parishioners to seek psychiatric help at Harlem Hospital, they often responded, “‘I’m not going there; they’ll strap me down on a gurney and have the police take me to Bellevue. And if I go there, they’ll send me along to Manhattan State Hospital, where I’ll never be heard from again.’”[3] While many local residents understandably feared entering the nearby Harlem Hospital or other municipal institutions, walking into the Parish House held no such threat or stigma.
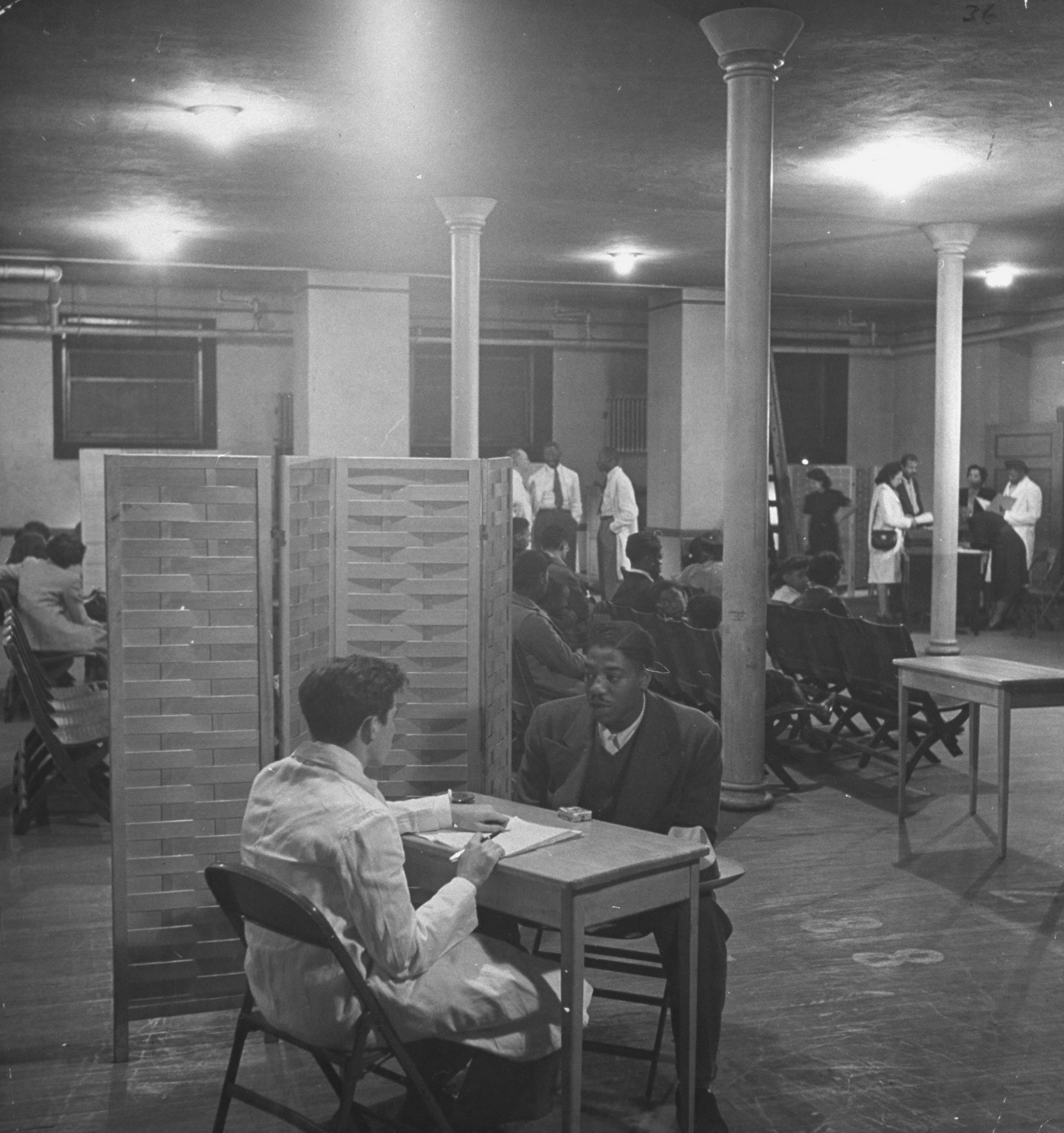
First-time visitors to the clinic would descend the stairs and find a busy hum of activity. Clinic hours were on Tuesday and Thursday evenings to encourage working Harlemites to attend. After checking in at the entrance desk, they would be directed to a specialized case worker to take their case history. Then, they would meet with a therapist who had some training in psychoanalytic methods. While traditional psychoanalysis tended to require 45 minute to hour-long sessions, three to five times each week, the clinicians modified the process to allow for shorter sessions — from 15 minutes to one hour, once a week. Most sessions took place in makeshift booths created by screened partitions.
A document outlining suggestions for the first session showed the importance clinicians gave to patient narratives. Dr. Luise Zucker wrote: “Establish a good working relationship with patient. This can be achieved by showing him both your sympathy and your respect for him as a human being. Listen carefully to what he says and how he says it. Take notes while patient is talking, not in retrospect. His own formulations rather than your own can be very enlightening.”[4] Her directive was followed by a list of points to cover, including the patient’s chief complaint, feelings toward their current job, family, marital, and education history, as well as fantasies and day dreams. Wertham encouraged staff to assess the social context of patients carefully and to consider even responses that might appear “crazy” to be based in a disordered society and not simply a disordered self.
Though the surviving case files of the clinic are not extensive, scholars have found striking examples of how the anti-racist psychiatry practiced by clinicians forged a distinctive approach to patient care. Therapists gave their patients space to talk at length about their experiences, and patients frequently identified racism as a central part of their psychological problems. Historian Catherine A. Stewart found that a young mixed-race girl’s file showed her acute awareness of the animosity between her white father’s family and her Black mother’s relations. Stewart suggests that in talking this over with a therapist, the emerging narrative “rescripted Black pathology as encounters with white pathology.”[5]
In Under the Strain of Color, Mendes recounts another case study that typifies the clinic’s attention to how race and racism conditioned the internal lives of New Yorkers. A six year-old Black boy visited the Lafargue Clinic in November 1950 because his school said that he had behavior problems, his parents also found him increasingly disobedient, he had started to have asthma attacks, and had begun to suck his thumb again. The clinician found that his family had recently moved away from Harlem to a white area in Queens. Case files show that his new white schoolmates had “expressed a fear that if they touched him they would turn colored. [Patient] very much disturbed by this.”[6] His mother also wondered if his new hostility toward herself and his father was coming from a growing dislike of their dark skin color, engendered by his new surroundings in a majority-white neighborhood. The clinician did not pathologize the young boy or suggest that the current conditions were tolerable for his psyche and that he should acclimate to them, but rather advised his parents that he should attend the interracial playgroup held at the clinic, so that he was not just surrounded by white children in his day-to-day life. Six months after he became involved in the clinic’s playgroup, his mother reported that he had stopped having asthma attacks and sucking his thumb. As Mendes observes, “the clinic did not adjust the child to anti-Black racism. Rather the clinic presented another mode of play and interaction for the boy, one that countered the hostility of his school and neighborhood environments.”
Furthermore, therapists observed how the strains of living on the bread line adversely affected patients’ mental health. The historian Dennis Doyle, in his work on the Lafargue Clinic, emphasizes how clinicians frequently intervened in material ways to aid patients.[7] Wertham saw psychiatry for the poor as intimately connected to social work, and Doyle relates a case in which a poor Black mother reported to the clinic with physical symptoms of stress and anxiety. Clinic staff saw that much of her anxiety came from housing insecurity and helped her to navigate municipal bureaucracy to get a New York City Housing Authority apartment. Once she and her three sons moved in, they helped her to find furnishings. Patients attending the clinic could receive both talk therapy grounded in psychoanalytic theory and material help to relieve the interconnected stresses of poverty and racism.
The Lafargue Clinic operated for twelve years, holding its final session on November 1, 1958. The Clinic’s legacy lives on beyond the walls of the St. Philip’s Parish House. Wertham gave testimony in numerous lawsuits emphasizing how segregation inhibited children’s health development and informed jurisprudence on desegregation in the 1950s. Along with the foundational work of Kenneth Clark and Mamie Phipps Clark — the first African Americans to receive psychology doctorate degrees, and founders of the Northside Center for Child Development in Harlem in 1946 — Wertham’s work was cited in landmark cases in the fight for school desegregation.
The Lafargue Clinic and the Northside Center for Child Development’s specific emphasis on community mental health needs also had a lasting impact on the connectedness of psychiatric care and public health in New York. In 1954, New York State passed the Community Mental Health Services Act, which established community mental health boards in cities across the state that could disburse funds to local mental healthcare providers. The Lafargue Clinic was denied funding under this act when they applied, and this financial setback — alongside Bishop’s retirement in 1957, and the deaths and serious illnesses of several staff members — contributed to the clinic closing in 1958. Under the new leadership of Reverend Dr. M. Moran Weston, the St. Philip’s Parish House maintained its place in Harlem as a center for community services and health programs directed by members of the St. Philip’s congregation even after the Lafargue Clinic closed its doors.
The conditions that necessitated the Clinic’s establishment have not been resolved. Ongoing gentrification threatens community rootedness. Social psychiatrist and urbanist Mindy Thompson Fullilove has worked extensively on the connection between neighborhood dynamics, displacement, and psychology. Her pathbreaking research on urban renewal efforts and dispossession in the United States identified what she terms “root shock,” and defines this phenomenon as “the traumatic stress reaction to the destruction of all or part of one’s emotional ecosystem.”[8] Based on her research in cities like Pittsburgh, Newark, and Roanoke, Fullilove argues that razing neighborhoods of color in urban renewal programs caused many residents to experience root shock.
Fullilove emphasizes that “milieu therapy,” which consists of environmental responses such as creating healing places that encourage community, is highly effective in treating root shock. But the most effective response would not necessarily come from licensed psychiatrists, but rather from urban policies that nurture and preserve neighborhoods. These policy interventions should be responsive to community members’ demands and needs, because community care is difficult to ensure when the community is constantly dealing with institutions’ insensitivity to the social and psychological impact of upheaval. Creating and maintaining places in which people can feel rooted is not only integral to mental health treatment in urban spaces, it is crucial to community belonging, wellbeing, and the preservation of working-class, multi-racial neighborhoods in cities.
Above, explore the Mental Health Data Dashboard, an initiative by the New York City Mayor's Office of Community Health to provide information on various social factors affecting mental health; unequal access to mental healthcare; and existing mental health services and support.
Renewed interest in the Lafargue Clinic’s influence showcases how the short-lived community care clinic’s philosophy resonates today, especially since the structurally racist processes that made the clinic necessary have not yet been abolished. Wertham and Ellison generated a space in which Harlem residents could respond to the trauma of displacement, the generational repercussions of root shock, and racial discrimination without fearing the stigma of naming these harms and their effects. The conclusions drawn from Wertham’s sessions with Harlemites were crucial to subsequent desegregation efforts because the clinic provided a space for the community to be heard and to seek accessible care that they could not otherwise afford, and Wertham used his privilege and expertise to elevate the community’s long-standing struggle to national attention. If we are to seriously combat the injustices that pervade American life, approaches to remedying harm should consider how to make spaces to combat exclusion, provide services that promote wellbeing, and generate political responses that can cement these strategies moving forward. Marginalized people’s exclusion prevents them from living “the good life,” one in which they have community, institutional support, and a place in which to flourish, which are basic necessities that should be promised to all. Wellbeing cannot be ensured in a community unless everyone’s wellbeing is equally valued and sought.
The authors would like to thank Gabriel Mendes for his input at the beginning of this project.
Cheryl Lynn Greenberg, Or Does It Explode?: Black Harlem in the Great Depression (New York: Oxford University Press, 1991), 60.
Ellison quoted in Gabriel N. Mendes, Under the Strain of Color: Harlem’s Lafargue Clinic and the Promise of an Antiracist Psychiatry (Ithaca: Cornell University Press, 2015), 116-117.
Ibid., 85-6.
Folder 12, Lafargue Clinic Collection, Schomburg Center.
Catherine A. Stewart, “‘Crazy for This Democracy’: Postwar Psychoanalysis, African American Blues Narratives, and the Lafargue Clinic,” American Quarterly 65, No. 2 (June 2013), 388.
Quoted in Mendes, Under the Strain of Color, 114.
Dennis Doyle, “‘Where the Need is Greatest’: Social Psychiatry and Race-Blind Universalism in Harlem’s Lafargue Clinic, 1946-1958,” Bulletin of the History of Medicine 83, no. 4 (Winter 2009), 759-760.
Mindy Thompson Fullilove, Root Shock: How Tearing Up City Neighborhoods Hurts America, and What We Can Do About It (New York: One World Books, 2004), 11
The views expressed here are those of the authors only and do not reflect the position of The Architectural League of New York.
In the face of exclusion and displacement, how do communities mobilize urban space for mental health and collective wellbeing?