We are celebrating 15 years — and counting — of stories that are deeply researched and deeply felt, that build a historical record of what the city has been.
We are celebrating 15 years — and counting — of stories that are deeply researched and deeply felt, that build a historical record of what the city has been.
The Narcotic City isn’t a master plan, or a map of where someone can access drugs, syringes, or safe consumption sites. For a collaborative of researchers, organizers, and archivists, it is a way to see how “the governance of narcotics play[s] a crucial role in the production and control of public spaces.” “Cultures of drug use,” the developers of the Narcotic City Project write, “are deeply interwoven into public spaces, everyday lives, and the contested governance” of cities in Western and Central Europe. Of course, public drug use is a longstanding matter of concern and conflict in New York City, too, where complex questions of health and safety, race and poverty, cut across streets, parks, and a housing system in crisis. Where anti-drug discourse and criminalizing policies have long dominated, there are growing discussions of safer consumption practices, or harm reduction. Typically understood as a set of public health practices to mitigate risks for substance users, harm reduction is beginning to appear as an actionable standard through allotments in federal, state, and city budgets.
Last fall the Narcotic City held a discussion in NYC on harm reduction, featuring activists and organizers who mobilize resources, operations, and outreach to provide safer conditions for practicing drug use. Bronx Móvil is a mobile collective that distributes clean syringes, condoms, sleeping bags, and food, and provides more easeful access to support for Puerto Rican drug-using communities in the Bronx and Upper Manhattan, taking to the streets after hours when health services are less frequent and accessible. The collective documents its regular routes with the same care and solidarity that informs its work. Through mapping and collecting qualitative data, it has developed a deep understanding of the shifting geographies and varied experiences of our narcotic city — information that can provide important insights both for those less familiar with the practices and consequences of public drug use, and those overseeing public health programs. In the interview below, co-founder Tamara Oyola-Santiago provides insight into Bronx Movil’s practices, some of the little-seen contours of New York’s narcotics landscape, and how spatially and culturally grounded knowledge can provide a road map to a more humane, drug-using city. – TG
How did Bronx Móvil get started? What needs did you see that were going unmet in the Bronx?
We started in 2018 as a group of people who live in the Bronx who are also harm reductionists. We knew that there was a need after hours, on weekends, late nights during the week, and holidays to provide direct services that would leverage public health tools such as syringes, naloxone, and fentanyl testing strips, but also nutritional support and urban living supplies, like sleeping bags, hand warmers in the winter, and socks year round. Our vision is that harm reduction must be 24/7 and also culturally and linguistically centered.
What we’re proposing is a harm reduction that is community-centered, community-led, and responsive to the needs of that specific community. Health on the streets must be in the language spoken by the community. If folks who are unhoused in the Bronx spoke other languages, such as Mandarin or Farsi, then community-driven and -guided harm reduction would need to be in those languages. In the Bronx right now, due to the dynamics of migration, colonization, poverty, racism, and many other oppressions, it is Spanish.
The founders are all Puerto Rican. We all have this experience of being from this community that has been deeply impacted by the War on Drugs. When you look at the people who are unhoused, unsheltered, and living on the streets of the Bronx, from our participants — at this point, we have over 1,500 — about 70 percent are Puerto Rican. Many of us have that lived experience of being impacted by being unsheltered, unhoused. We move in solidarity because our community is impacted for a multiplicity of reasons.
Bronx Móvil is made up of a beautiful community of harm reductionists. We have folks who are survivors of the War on Drugs, people who are formerly incarcerated, folks who are currently living in the shelter system. We have others that are academics, that have graduate degrees, and then others who have a GED or a high school diploma. We have migrants; we are multiracial and Black, we have white comrades and allies.
Bronx Móvil is constantly and literally on the move across the Bronx. Even though not every day is the exactly the same, what does a typical day look like? And what do you see on the road?
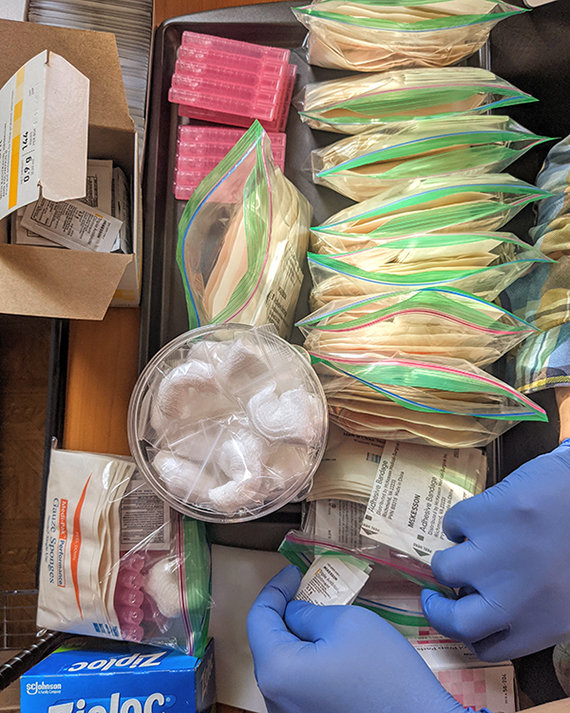
This group of beautiful harm reductionists come together on Saturday nights, Sunday days, holidays, and Monday evenings. It’s mobile, so we don’t have an office. We’re operating out of my apartment. If we have to use the bathroom, we go back to the apartment, and then we hit the streets again. We pack a car with anywhere between 50 and 80 bags with syringes, wound care kits, safer injection kits, safer smoking kits, socks, bottled water. The St. Francis Breadline in April 2020, started giving us about 100 sandwiches each weekend, plus juice and snacks, and they haven’t stopped. The Migrant Kitchen has been donating food as well. We’ve been able to include other surgical masks and hand sanitizers since the pandemic started. A grant from AIDS United allowed us to purchase our own vehicle, but before, via mutual aid, we rented a car. There’s a team of three to four of us that then hits the streets.
We’ve been doing this work for almost five years. Our catchment area is all of the Bronx and Washington Heights in Manhattan. In the very beginning, we knew there was a need, but we weren’t exactly sure where: where are the nighttime fixed encampments, or where folks move due to police presence and sweeps, and how they move around depending on the weather. At this point, we have established routes that are flexible. We know that in this particular area, underneath this one bridge for example, there tends to be a community. So we’ll go there, park the car, and walk. And if we don’t see folks, we move around, we drive around until we find them.
We don’t end until we have distributed all of the bags we prepared for the day. With the winter, we’ve been going out around 2 pm because it’s getting darker earlier, and we’ve been giving out about 50 to 60 bags. In the summer, we’ll start going out on Saturdays around 4 pm, but we’ll go out all the way to 11 pm, if not midnight. It’s hot, people are out and about. We may go from seeing 50 people in the winter to seeing 100 people on a summer night. It really does depend on where people are, and where people are is going to depend on the weather and on the presence of police and sweeps.
The Bronx is being hit hard by gentrification. Gentrification is very violent, and it leads to displacement of those New Yorkers that are most vulnerable, who are unhoused and living on the streets. We see constant sweeps that include sanitation and police, where people are displaced. They throw away people’s belongings, who have so little to begin with. All you need is a sweep to come through, and there goes the sleeping bag, right? So in the winter we’ll give out as many sleeping bags as we can.
Gentrification is creating a forced migration of people throughout the Bronx, going from the south to the north, because in the south you have Harlem, which is like ground zero for gentrification. There are layers to this displacement. For unsheltered New Yorkers it means moving into areas where there is some privacy, like under bridges, tunnels, parks, scaffoldings; all of these offer some privacy as well as shelter from the elements. For others, it is sharing housing with multiple folks in a room. In all of these cases, what we see is that home requires community and our folks create that home wherever they can.
Our philosophy is that harm reduction has to be able to meet the needs of people where they’re at. When talking about “where they’re at,” which is a harm reduction pillar, usually people mean “where they’re at” psychosocially. But we also mean it in real-time and real-place. Because if you’re asking somebody who is living on the streets with very limited economic means to get on the subway, to get on the bus, to actually mobilize in order to access your syringe service program, or your clinic, or your medical service, can they afford it? If they leave, will sanitation come and throw away their belongings? What is lost by asking them to come to you? What is gained by coming to them?
Health services in general should be mobile, should be meeting people where they’re at in terms of time, place, location, psychosocially. I think that kind of ‘checking ourselves’ with regards to economic privilege and access to services is something that we have to deal with in public health and medicine.
You mentioned just now the harm reduction principles that Bronx Móvil has. How would you define or describe harm reduction?
You can go at it two ways. I can use the traditional definition, which basically says that harm reduction is a set of public health tools that reduce both risk and harm related to both HIV and hepatitis C. These tools include syringes, cookers, and wound care materials. Harm reduction is also the movement by and for people who use drugs. This movement seeks to end the War on Drugs. Many of us live with racism, and sexism, and trans- and homophobia, and discrimination based on ability, class, migration status. The -isms create this systemic oppression that stigmatizes and criminalizes drug use. Harm reduction is a movement created by people who use drugs that uplifts and says, “Look, we take care of each other. We take care of each other because the systems have failed us repeatedly.” I think in order to do true harm reduction, you need both, that radical love, as well as the provision of these tools that save lives.
I will add to all this that harm reduction needs to be liberatory, and part of the liberation is an examination and action to address the dynamics of power that happen within a movement. For example, right now we have successes, such as the Biden administration embracing harm reduction and mobilizing funds at the federal level, but we still have the War on Drugs and the criminalization of drug use, which due to white supremacy and racism impacts BIPOC and poverty-impacted communities. The War on Drugs criminalizes poverty.
In addition, if funds are funneled through agencies that use that biomedical model and lens of addiction, then in some ways, we might be leaving out true harm reduction that says, “You decide.” Some of us in harm reduction don’t say “addiction,” because that word carries a stigma. We say “people who live with a substance use disorder” or “people who use drugs.” People, as part of their own sense of agency, have to name themselves and their use — or not.
We can also talk about drug use as pleasurable, as something that brings people together, that gives comfort, that establishes loving, close relationships and dynamics of support. If we’re only able to talk about the stigma and about the negative aspects of drug use, we will never be able to comprehend the full human experience with drugs. That limits our ability to create programs and services that uplift the humanity of individuals. Drug use is a spectrum: some of it is problematic, some of it is not.
You were talking earlier about the importance of mobile services. A lot of the work you’re doing is in the after-hours, it’s in the conditions in which harm reduction, as it currently is modeled, is not able to reach people. They’re very medical, they’re very traditional, public health-oriented, and operate during ‘business hours.’
I’m not saying that brick-and-mortar public health, building-specific harm reduction, is not needed. Over time, though, that biomedical model has become the dominant model. This model requires a robust clinical setting with a lab, being able to bill for services: an infrastructure that supports the building. And brick and mortar sites for the most part operate 9 am to 5 pm on weekdays. I want to be able to refer people who are ready for whatever services are needed, whether they be mental health, physical health, detox, rehab, at all times. My participants request support 24/7, so why isn’t the system built with this expansiveness?
When I’m out there on a Sunday morning at 8 am, what is available to me for detox rehab is very limited. We have had to tell participants to wait until Monday morning so that they can be the first in line when the detox rehab opens up. And let me emphasize this is in particular an issue for people with limited economic means that depend on public medical insurance. We need to be creative as a movement of public health and really think about who has access to what, and at what time?
How does harm reduction policy inform your practices in urban and public spaces? How does the current policy that exists inform the hours, the places where you’re able to operate?
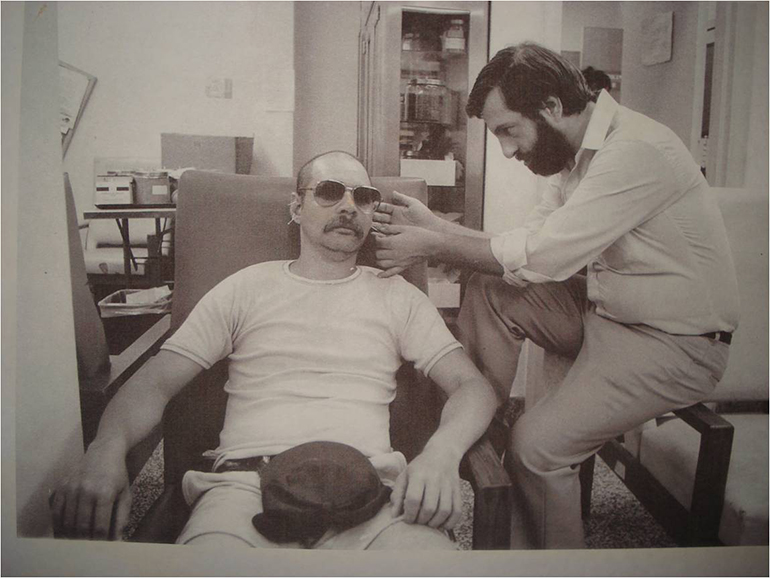
In New York State, we have very robust harm reduction services and programs, for example, where collectives have access to free syringes and safer injection materials. State supported syringe exchange and services are available because of the organizing and activism of HIV/AIDS and LGBTQIAGNC activists, like Keith Cylar and Brian Weil and Iris de la Cruz, early harm reductionists who pushed and fought like hell for services, treatment and respect. I always like to mention the Black Panthers and the Young Lords, movements based within communities of color that were like, “Yo, there’s a heroin problem going on in our community. Let’s figure out what to do about this.” There’s been a rich tradition of Black, Indigenous, and People of Color harm reductionists. For example, the Young Lords and the Black Panthers, brought acupuncture based detox to their Black and Puerto Rican communities in The Bronx and Harlem, and elsewhere.
I think that this gets at a misconception, too, about harm reduction. The Black Panthers and Young Lords were some of the first groups that brought harm reduction to Black communities in Upper Manhattan and the Bronx. There was a recognition: “We don’t want just a bunch of methadone, we want other avenues of being able to demonstrate health practices in our communities. We want food.” The same thing with safe injection facilities: It’s a place for people to inject safely, but it’s also a place where people’s names are known, and they can be greeted, and there’s people with warm, friendly faces. All of those other things are the ability to have harm reduction be effective and impact people’s lives.
I always say, in the process of harm reduction, it’s about a reciprocal, symbiotic, gorgeous dynamic of humanizing each other, of being able to recognize the humanity of those of us that do the work, and also those of us who are receiving. It’s continuous. Those of us that are providing are also receiving.
A lot of the work you do with deciding on the routes that you go on is based upon the visibility of where your services are needed, the relationships that you formed, and the knowledge that comes in those conversations. People that you work with telling you which areas may be best served on the day that you’re in. All of that is important and valuable knowledge. With your research, you’re also cultivating and gathering information that otherwise would not be there.
From the beginning, we thought it was important to go beyond the quantitative, which is what funding typically requires. We decided to take what we call ethnographic notes of what we are seeing. So syringe littering, encampments, police presence. We’ve seen stop-and-frisk stops, and have had to call 911 upon request by participants who need urgent medical care. We advocate and triage. We document these quality-of-life indicators that are happening as we do the outreach. But we do that without recording any personal-level data. We keep the anonymity and confidentiality of our community, of our participants as much as possible.
The second level of data is quantitative. It includes number of syringes distributed, smoking kits, wound care kits, etc. We also engage with folks who are not using drugs, or maybe using but not injecting and want a sandwich, a sleeping bag, pair of socks, etc.
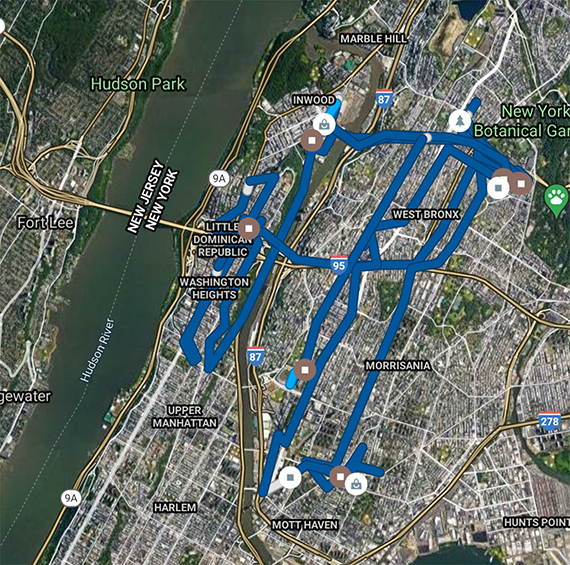
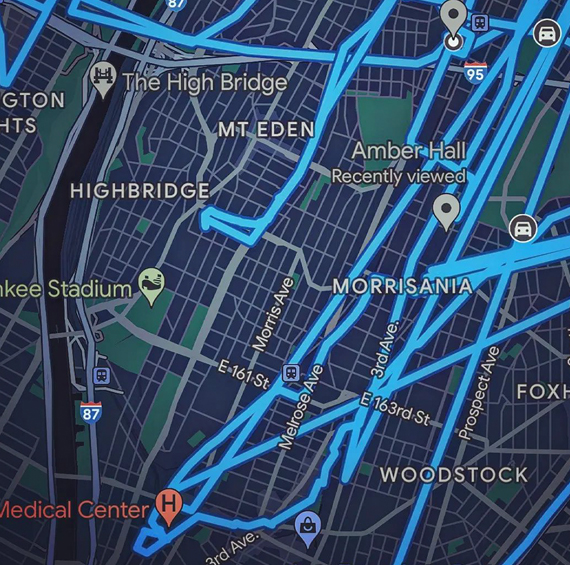
And then last, but not least, is geomapping. We don’t have funding for data collection and analysis, so we’ve had to be creative and use free platforms. We use Google Maps for our outreach routes. The routes combined with the ethnographic notes help us identify trends of gentrification, high areas of need and what is needed and where.
What does our community look like under siege by capitalism and by gentrification? What does it look like to actually live on the streets? We try to avoid trauma porn as we answer these questions. Because in many ways, what mainstream media does — and I would even say that some harm reduction organizations are guilty of this — they document the trauma of drug use and drug addiction, and in the process, they dehumanize participants.
Bronx Móvil has been very intentional around addressing the question of how we document our work, but also honor the dignity of those of us that are doing the work The collective itself is made up of people who use drugs. Many members of the people who do the outreach are also participants. So from the beginning, we were able to say, “How would you capture our work?” Not from the outside as a researcher, but almost like, how would I want to capture what I do. I think that’s really important, to say that the collective itself, which is made up of folks who are also participants, decide what the data metrics should be.
This abstracted concept of the Narcotic City is a way of capturing the totality of services and interventions, good and bad, which impact substance users and health care workers, including harm reductionists, and is a helpful lens to capture how the world of substance use is governed, practiced, and responded to. But in another sense, the Narcotic City is painfully grounded to include the spaces that harm reductionists and individuals must navigate to receive public services and basic care, including safer supplies, food, housing, and warm clothes. With this grounded and abstracted lens, how does Bronx Móvil — as a coalition of activists and harm reductionists, researchers and community members — experience the Narcotic City? And how would you use this lens to describe what you witness and intervene with your mobile outreach program?
That’s a hard one to answer because my reaction is one of sadness. It’s a painful city. The city hurts, the city is super violent. There’s a lot of pain inflicted between human beings, and also within operators of the system itself. Bronx Móvil sees a lot of pain: physical pain, mental pain, trauma.
In the pandemic, when many of us sheltered at home, we left people who live on the streets behind. We left them to shelter in their homes, and their homes were the streets. To this day, in the narcotic city, there are remnants of what it means to be abandoned in the middle of a pandemic. In the middle of the pandemic, Bronx Móvil would be the only ones, for weeks on end, doing street outreach. Covid hit us hard. We’re not laying blame. But as a movement, we failed to be creative on how to provide services that were not brick and mortar. We failed. The participants feel that deeply, still, in 2023.
Our community knows how to live with and thrive through pain. What we do within harm reduction is that through that pain, we try, there is an attempt to humanize and be able to say, “You are beautiful, you are worthy. You are loved.”
I don’t like to use the military language of warriors, but in some ways, we go in full armor. We go in with these vests of love because we might be experiencing that trauma, that pain, but we have been able to find a way to mobilize within that that says, “Yo, come here. We can do this.” It requires a community. One person doing the work is going to burn out, and we don’t need martyrs. What we need are people who come together and create families of support.
All photos courtesy Bronx Móvil and Tamara Oyola Santiago unless otherwise noted.
The views expressed here are those of the authors only and do not reflect the position of The Architectural League of New York.