



Series
Profiles in Public Service
Conversations with public servants illuminate the complex workings of city government and how local agencies shape the physical and lived experience of the city.
We are celebrating 15 years — and counting — of stories that are deeply researched and deeply felt, that build a historical record of what the city has been.
Protecting and bolstering public health requires attentiveness to hundreds of factors. Rats, noise, health insurance, fruits and veggies, and transportation infrastructure are all of interest to the NYC Department of Health and Mental Hygiene. And understanding and combating spatial inequity in health — that youth in East Harlem are more likely to end up in the ER from an asthma attack than those living 30 blocks south on the Upper East Side — are the charge of the agency’s new Center for Health Equity.
Marlon Williams, an urban planner and economist with previous stints across the city’s bureaucracy, works out of the center as the health department’s Director of Cross Agency Partnerships. Williams brings a keen understanding of how issues relevant to New Yorkers cut across agency specialization and a commitment to instilling a concern for health outcomes across those divides. In this installment of our series of Profiles in Public Service, Williams explains how the city’s built environment impacts health and lays out the challenges and promise of cross-agency collaboration that meaningfully integrates true community engagement. –J.T.
What do you do?
I work as the Director of Cross Agency Partnerships for the New York City Department of Health and Mental Hygiene in the Center for Health Equity. I focus on understanding the priorities of different City agencies and promoting ways to more intentionally support community health in their work. It’s about maximizing opportunities to direct existing resources towards improving health across the city in a way that supports all of our departments’ goals. I like to say that I’m advancing a health-in-all-policies approach.
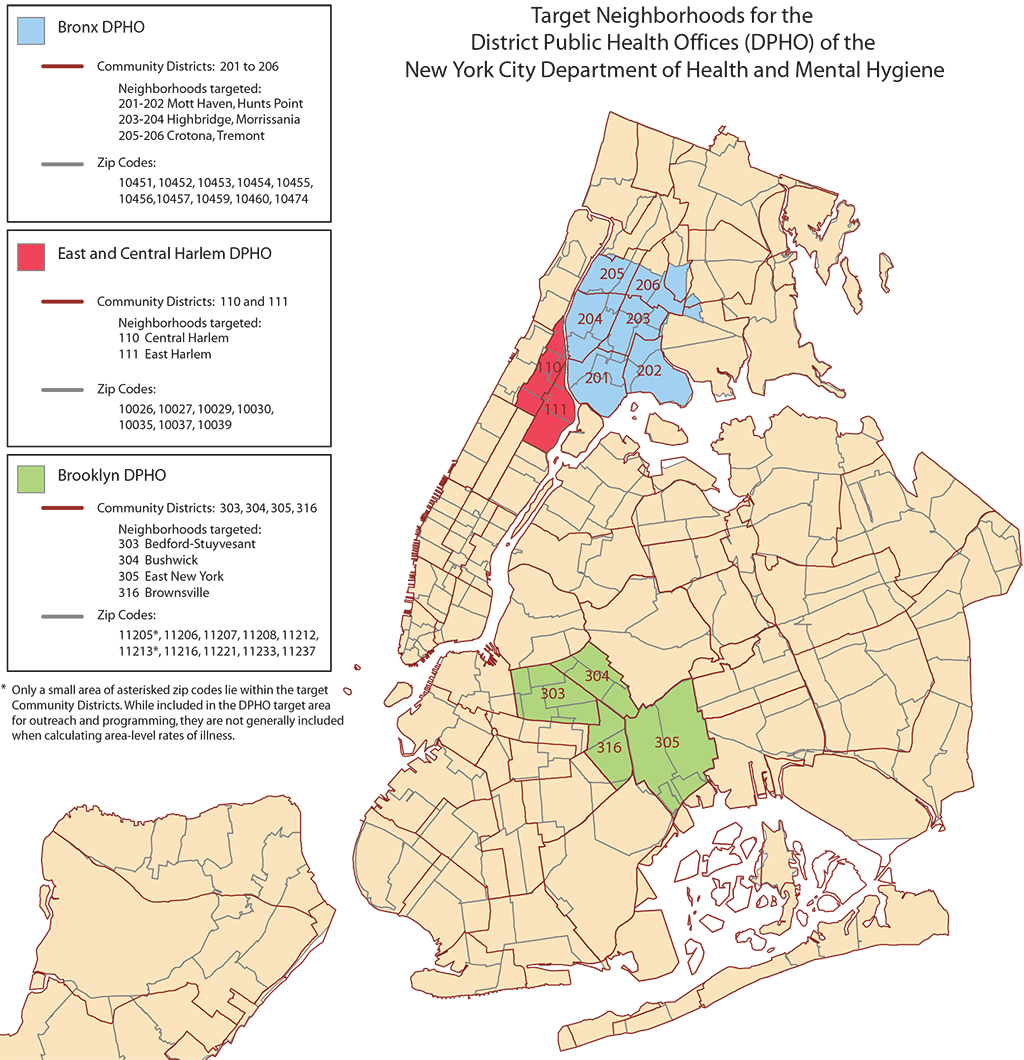
At the Health Department we have two key assets: a world-class capacity for research and analysis and a great information distribution mechanism to tell people what we’ve learned. We have district public health offices in the South Bronx, East and Central Harlem, and Central Brooklyn on which we build the foundations of much of our work. Each of these responds to different health needs within each community by using data and research and the amazing self-knowledge of community members. Right now there’s a lot happening in East Harlem: we’re coordinating planning resources, health programming, and a lot of existing community work to improve health, including a center that’s focused on asthma.
What do you mean by a “health-in-all-policies approach”?
No matter what we do there is a connection that can ultimately be made to health. Very few health outcomes actually have to do with your access to healthcare services. Much of what determines your ability to live to your fullest health potential is about the physical and social context in which you live. Issues of race, discrimination, class, and poverty all have a tremendous impact on health and create specific health inequities.
We know that those inequities are often concentrated within certain populations and specific places, but those linkages aren’t always so clear. Part of my work is to make those visible, including conducting the research that validates and explains them. We then try to figure out a place-based intervention to address, mitigate, or even prevent those issues — so anyone anywhere in New York City has an opportunity for optimal health.
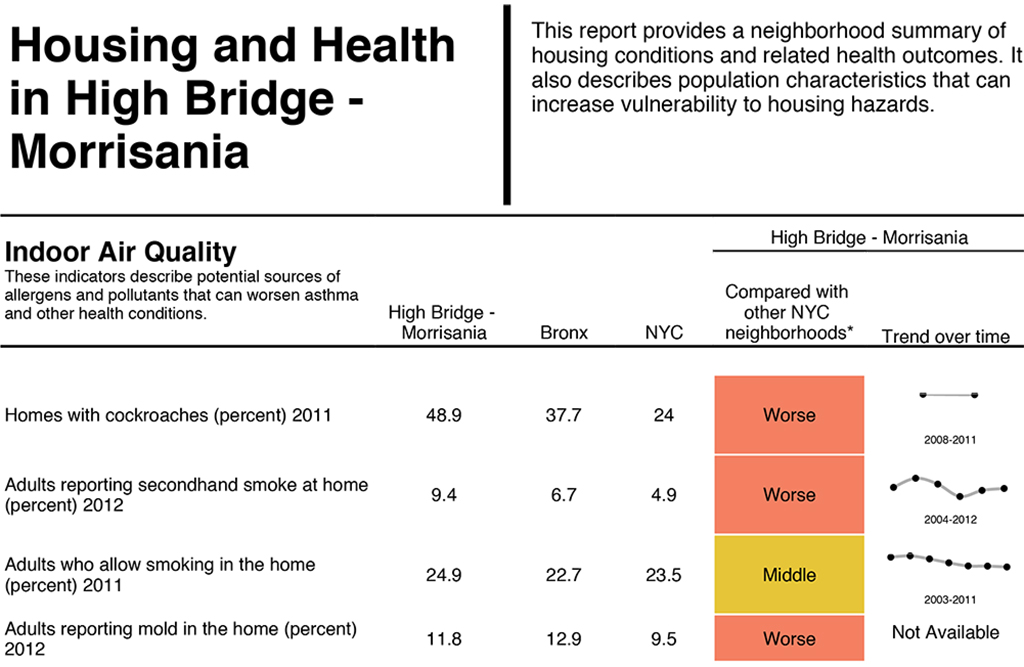
The Department of Housing Preservation and Development is one of my favorite partners because there is so much about where you live that has an impact on health — the quality of the air, the sense of safety, design elements that support people using the stairs rather than elevators. HPD has done an amazing amount of work to show that just by moving into affordable housing, the health of a family improves over time. That’s in part because of the affordability, and also due to high design standards that support health, like air purification. They want to create as much affordable housing as possible and as many healthy communities as possible, and it’s all about seeing that work as related.
Much of my work is about mindset change, but the goal of that is not just to get people to thinkdifferently but to also do differently. And there have been some recent policy changes that allow us to get results on a wider scale. For example, under the State’s Delivery System Reform Incentive Payment (DSRIP) program, how medical providers will be reimbursed by Medicaid is going to change. The old idea was that hospitals got reimbursed for the services they provided to people who came in for care. Under the new system, medical institutions will be incentivized to deal with wider community health and give attention to all the social and physical determinants of health beyond strictly traditional healthcare — the built environment, social services infrastructure, housing. I think this greater focus on prevention will lead to a lot of great changes in the provision of services around community health.
What areas are you focusing on right now?
I orient our work in four buckets. The first is food access. We want to make sure that healthy foods are available and affordable in every community. That is in part an infrastructural question. So if a new affordable housing development is going up, we might want to encourage a preference for a healthy food retailer in its ground floor space. We also have to work on the demand side to make sure the food is something that the community wants and is culturally relevant. We’ve had too long a history of saying this culture’s food is healthy and that one’s is not. We have to make sure that we’re responsive to community feedback in promoting healthy food.
The second bucket of work is active living. How do we design the urban environment in a way that encourages people to be active within their communities? In my head I have a mini-calorie counter, and I walk through the world looking for little tweaks we can make in the built environment so it supports someone to spend more calories here or there. The Department of Transportation might have a mandate to build X number of miles of new transportation infrastructure, and the way that is built impacts how we navigate through our city and the opportunities for active transportation, like walking and biking. A great example of this kind of thinking in practice is the Department of the Aging’s work with the Parks Department to install more benches in certain parks. Elderly people will walk more if there are more places along the way for them to rest. That’s a great health improvement that came from an infrastructural improvement.
The third area is economic development. There is a strong connection between poverty and health outcomes. In our health system, healthcare access historically has been connected to a job and it’s expensive. Within a family budget, money is transferable — if you can increase income or reduce costs, you create more space for people to invest in their health. That also means they are more able to work. The paid sick leave law that recently passed is a great example: taking the day off to rest or help sick family members allows employees to be more focused at work and more productive. They are only absent for one day and won’t then make others sick. You’re increasing overall productivity.
The last bucket is more generally creating connections to various resources. Being new to the health field, and coming in as an urban planner who has done a lot of economic development work, I see many resources that can support health that aren’t well coordinated or seen as such. So we’re trying to do the coordination work and facilitate access to those resources.
You’ve served in a number of roles in city government — what led you into a career in public service?
Ever since my family moved here from Guyana in the early ‘90s, I knew I wanted to make an impact on the city. I initially thought I would make lots of money in finance and then try and help in some way. But in college I attended a study abroad program that took me to India, South Africa, and Brazil to study urban planning.
At one point I was living in the townships outside of Cape Town, South Africa. My host parent had lived through apartheid, built her own house, and graduated from college at age 60-something. I asked her why she stayed there even though she now had the opportunity to move into the city. She said that we were given a place that was nothing, and we made something of it; by building a community you can take places that seemingly have no value and see the value that’s there. I’ve been spending the rest of my life trying to figure out what that means and how to do that.
The central question is, how do you create communities where people have an attachment to each other and to the place? A lot of my earlier work was focused on housing — where people live and how people live together. I used to work for the Department of Housing Preservation and Development. From there I had the amazing opportunity to work under Linda Gibbs, the Deputy Mayor for Health and Human Services in the Bloomberg administration, who taught me about the real need and opportunity for coordination between City agencies. In my last position at the Human Resources Administration, I headed up Jobs Plus, a workforce development program for residents of public housing. I’m still working with my former staff to get more people employed so they have access to healthcare as well as to make sure that healthcare providers, which are large employers in many neighborhoods, hire locally. They then provide healthcare for residents who ultimately become employees and tap into resident knowledge to best deploy services in the community.
Is this desire and concern for working in a cross-agency and cross-disciplinary manner new or growing in city government?
For a time each agency was focused on doing its own work and organizing its own internal processes better, and you had to make the argument for collaboration. But we’re beyond that and now we’re more concerned with how to make collaboration more effective. We’re doing a better job of aligning our interests when we’re working in the same place, saying “Hey! You’re over there building infrastructure. I’m over here building social services. How do we make sure your infrastructure gets people to my services?” The next level is asking if there is something new and different outside of our silos that we could do together to have maximum impact.
The way we structure city government is about specialization, but that’s not how we live our lives. Neighborhood issues aren’t about specialized areas, but things that cut across.
Safety is about the quality of infrastructure, community cohesion, policing and relationships between police and the community, economic development, physical spaces, and social services. But there’s no agency for safety; it cuts across. So, my work asks how we build on the value of specialization while orienting that in a way to best support families.
How does such cross-agency partnering work in practice?
It’s all about building relationships and networks. In my experience, there’s definitely been top-down support for this approach — commissioners are supporting and asking for collaboration. At the grassroots, communities really understand that their issues span different agencies and they’re demanding city government be responsive in that way. But there’s also a third level that’s not always talked about, and that’s people like me within city government who are switching agencies much more, learning and building relationships at each. There’s cohesion among people who have worked at different agencies and we are creating the demand and the backbone needed to support and facilitate cross-agency collaboration.
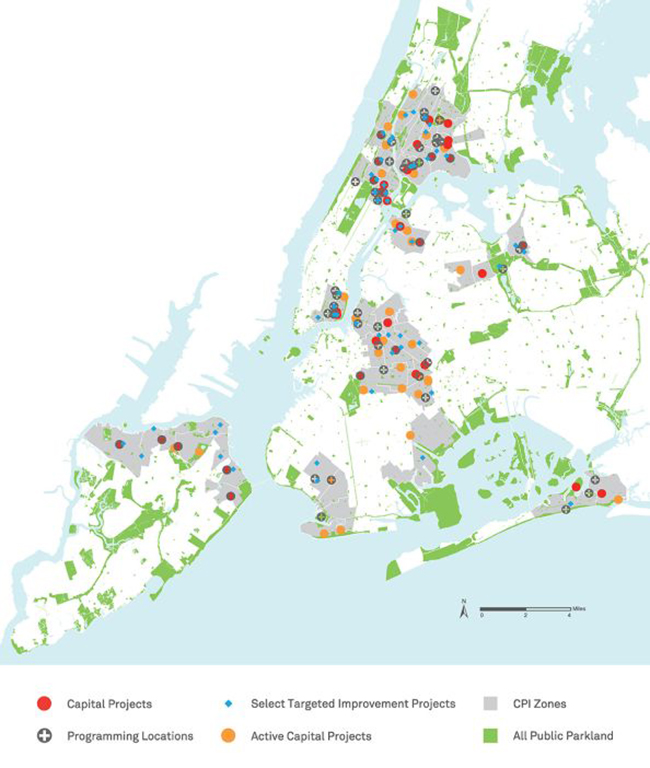
Some of our work is just about taking a step back to understand what everyone is doing so that we can identify synergies and amplify and support each other’s work. For example, citywide efforts like the Community Parks Initiative, an investment initiative in smaller public parks in areas of poverty concentration, extends beyond the Parks Department. You want to bring in the Department for the Aging because a lot of park users are seniors. Many local parks are next to schools and public housing, so you bring in the Department of Education and NYCHA. We want people to be active and to track that, so you include the Department of Health. There are safety implications, so you bring in the NYPD. A revitalized neighborhood park might present an economic development opportunity, so you include the Department of Small Business Services. It balloons out, but in a good way.
Are there projects you are particularly excited about right now?
I’m really interested in how we develop our bike infrastructure in a way that’s equitable, that it reaches neighborhoods where the impact might be greater. That involves changing the frame so that this infrastructure is recognized as a resource for the community rather than an outside, gentrifying force. We should recognize that within many communities there are bike cultures that look different than the ones traditionally advertised. We need to activate those and think about the infrastructure not as a way to get through the neighborhood, but as an amenity that can and should be used by people in it. Then a conversation about biking might transform into one about public safety and how people feel navigating through the neighborhood, which we can use to identify design and safety elements to improve that. We had a great experience with that work in Central Brooklyn — by bringing the community into the planning process, the DOT was able to build out many more miles of bike lanes than had originally been planned and the process led to greater utilization.
So ultimately what I’m excited about is that our ideas around community engagement are becoming much more sophisticated. I think there was a time when community engagement meant we hosted a listening session, and then we went and did what we were going to do anyway. That’s no longer acceptable. We’re making sure community engagement is a real thing, where we deal with issues of power and privilege and try to make it a process that really does transfer power to people who may not have had as much of a voice in the past. We want to activate community voice, community knowledge, and community power so that the planning process, resource allocation, and decision-making in city government resonates with the community and achieves greater impact.
The views expressed here are those of the authors only and do not reflect the position of The Architectural League of New York.
Conversations with public servants illuminate the complex workings of city government and how local agencies shape the physical and lived experience of the city.