We are celebrating 15 years — and counting — of stories that are deeply researched and deeply felt, that build a historical record of what the city has been.
We are celebrating 15 years — and counting — of stories that are deeply researched and deeply felt, that build a historical record of what the city has been.
Across New York City, a certain kind of medicine is administered not in a regular pharmacy or a doctor’s office, but in its own kind of space altogether. Most often, these are brick-and-mortar locations, clustered in lower-income communities of color; increasingly, such treatment sites are mobile and distributed. In either case, one specific type of person seeking medical care is being segregated from nearly all others. Opioid addiction may have received more attention in recent years, but the geographic footprint and spatial practices of methadone maintenance treatment remain hyper-concentrated and sequestered. Communities such as Harlem are overburdened with facilities providing care for a large proportion of the city’s estimated 28,500 people in recovery; yet there are very few methadone clinics to be found in wealthier, whiter neighborhoods such as the Upper East Side. Meanwhile, patients themselves have long borne the brunt of controversy and conflict with neighbors and the state alike, compounded by familiar vectors of discrimination and policies that conflate disease with crime, and treatment with punishment. As the City opens the country’s first officially-sanctioned supervised injection sites, charting a new direction in harm reduction, Zoe Adams explores the fraught history of New York’s methadone clinics, and questions whether one particular form of healing needs its own separate space in the first place.
Syderia Asberry-Chresfield is on a crusade against the overwhelming presence of methadone clinics in her neighborhood. A Black woman in her sixties, and an owner of a historic brownstone about one block west of Marcus Garvey Park, Syderia moved to Central Harlem from Queens in 1995 after coming across an article in The New York Times in the late ‘80s encouraging readers to buy homes in Harlem. Syderia jumped at the chance, she told me, because Harlem was “changing and I wanted to be a part of that change.” When I met Syderia at her house, a pink-and-white “Home Sweet Home” doormat greeted me at the top of her brownstone’s exterior stairs. A sign in her front window reads, “SMILE, YOU’RE ON CAMERA.” A thriving community garden — which Syderia helped revive after part of a neighboring building collapsed into it a few years ago — stands opposite her house. Her brownstone, which received landmark preservation status last year, is a fortress to the Harlem streets that no longer bring her joy.
Syderia characterizes the presence of methadone clinics in her neighborhood in warlike terms. In a letter to the New York State Assembly advocating for a reduction in density of methadone clinics in Harlem, she refers to herself and her neighbors as “besieged” residents fighting to end “the structural racism that confronts us every time we leave our homes.” Methadone clinics — with their long public lines, mandated daily dosing schedules, and street-level, unmarked facades — seem more like parole offices than spaces that provide medical treatment to patients. To Syderia and others, methadone clinics attract criminal behavior and fuel racist stereotypes about Harlem that residents have been trying to shake off for decades. Where else in Manhattan but Harlem would spaces like these be permitted to exist?
Syderia is a co-founder of the Greater Harlem Coalition (GHC), an organization of over 6,000 residents and community leaders devoted to improving quality of life and safety in Harlem. According to Syderia, patients from all over the city commute to the neighborhood to “anonymously get their treatment outside of their community.” In 2018, GHC members successfully prevented the opening of a methadone clinic that would have demolished a historic brownstone in Harlem’s Sugar Hill neighborhood. Before COVID-19, Syderia led tours of Harlem’s brownstones (her house was featured one year) because she wanted “people to see how beautiful Harlem was.” She pauses here and shakes her head, almost disappointed with herself for using the past tense. “How beautiful Harlem is.”
Mount Sinai-Beth Israel, an academic medical center whose presence can be felt across the city, operates two methadone clinics a ten-minute walk from each other in Harlem, which serve approximately 2,400 patients. Before I visited these clinics, Syderia warned me of a key detail. The publicly listed addresses for the clinics were the entrances for staff and administrative personnel. Patients had their own entrances, and these building numbers were unlisted. Two yellow-jacketed security guards strategically positioned themselves around a clinic located at 1865 Park Avenue. One guard stood in front of the patient entrance, and the other manned the block closer to the entrance for staff. Police presence is typical at these clinics: across the US, law enforcement officials have arrested and harassed patients waiting in line to receive their medication. I had to confirm with one of the guards that the unmarked entrance was actually a methadone clinic, as there was no signage saying so. To utter the word “methadone” made me feel like I was telling a secret or disclosing a highly protected passcode. I could only imagine how patients felt.
In the early 1970s, when methadone clinics began cropping up across New York City, Ithaca Medical Center, a private clinic on East 84th Street, was forced to move to East Harlem after white residents’ demands for the clinic’s relocation were backed by US Congressman and future New York City Mayor Ed Koch. According to physician-anthropologist Helena Hansen and historian Samuel K. Roberts, methadone clinics were more likely to proliferate in predominantly brown and Black neighborhoods, where “local opposition [was] less organized.”[1] This unevenness persists today: a 2016 study revealed that U.S. counties with highly segregated Black and Latino communities had significantly more methadone clinics per capita compared to white communities. White communities instead had more facilities that provided buprenorphine, a less regulated treatment for opioid use disorder (OUD) that can be prescribed in a doctor’s office and picked up at a pharmacy.
In their attempt to protect property values and maintain a “vibrant, tolerant, clean, and safe” Harlem, movements like the GHC can have the damaging side effect of dehumanizing people who take methadone and people who use drugs. In seeking to distribute methadone clinics more equitably across New York City, the GHC has prevented the opening of clinics in Harlem, decreasing access to methadone and contributing to the stigma that patients on this medication face on a daily basis. In 2020, overdose deaths hit a historic high of 93,000 in the US — the largest single-year increase ever documented. Only 18 percent of patients who have been diagnosed with opioid use disorder (OUD) take either methadone, buprenorphine, or naltrexone, the three FDA-approved medications for the treatment of OUD. Methadone, the oldest and most stigmatized of the three, prevents people from dying from overdoses. It has a longer half-life than most opioids and can stabilize patients by preventing withdrawal symptoms; methadone also decreases the risk of HIV and Hepatitis C infections, and is correlated with improved quality of life as well as physical and mental health outcomes. Syderia believes in methadone as a treatment — she considers addiction a chronic disease and methadone as “just another form of medication.” But it is the medical redlining and “dumping on Black people” that she can no longer take. Improving access to methadone doesn’t have to mean building more clinics. In fact, the clinic system — a geographically concentrated and racially segregated approach to distributing medication that stigmatizes patients by design — shouldn’t exist at all.
In the early 1960s, as a heroin addiction epidemic devastated communities across the US, government officials and members of the scientific community were eager to establish effective out-patient treatments.[2] Starting in the mid-1960s, methadone maintenance treatment (MMT) was becoming increasingly accepted in scientific circles due to promising, yet controversial, clinical trials conducted at The Rockefeller University Hospital in New York City. A study published in 1965 in the Journal of the American Medical Association demonstrated that methadone decreased cravings for heroin and allowed patients, according to the study’s authors, “to live a normal life.”[3]
Early scholarship on methadone echoed the racialized rhetoric of the “war on drugs.” Methadone was determined to be an effective medication partially due to its association with crime reduction, especially among young Black men.[3] Under the Nixon Administration, the Food and Drug Administration (FDA) approved methadone for the treatment of opioid addiction — previously, methadone could only be used to treat chronic pain or given in short courses for opioid withdrawal — and with this came stringent regulations that continue to influence how methadone clinics shape the places and identities of the patients they serve.
In the 1970s, medical and law enforcement agencies did not view or fully embrace addiction as an illness. Debates about the nature of addiction — which some groups understood as a chronic disease, and others as a moral failing with abstinence as the only solution — were reflected in the physical spaces that provided methadone. The new regulations assumed people taking methadone were criminals, the types of people who substituted one drug for another and would illegally sell their methadone on the street to make a profit. People taking methadone weren’t quite considered patients, so a traditional clinic would not suffice. The spaces that provided methadone had to be something else. The FDA mandated that patients on methadone report to designated distribution sites, known as opioid treatment programs (OTPs), almost daily to receive their medication. Patients were required to line up publicly outside of the OTP and stick out their tongue while being watched to ensure their methadone dose was swallowed. Patients had to undergo punitive weekly urine screens (if patients tested positive for another substance they could be kicked out of the program) and required counseling sessions. Many of these requirements, with slight variations depending on the state, persist today.
Ed Koch’s 1974 takedown of an Upper East Side methadone clinic is just one example of a broader backlash against these clinics. Since methadone clinics were first established in New York, community pushback and frequent, invasive federal audits have done more than stir up local tiffs: they’ve incited violence, protests, and left an indelible mark of stigma on the patients who must show up daily to get their doses.
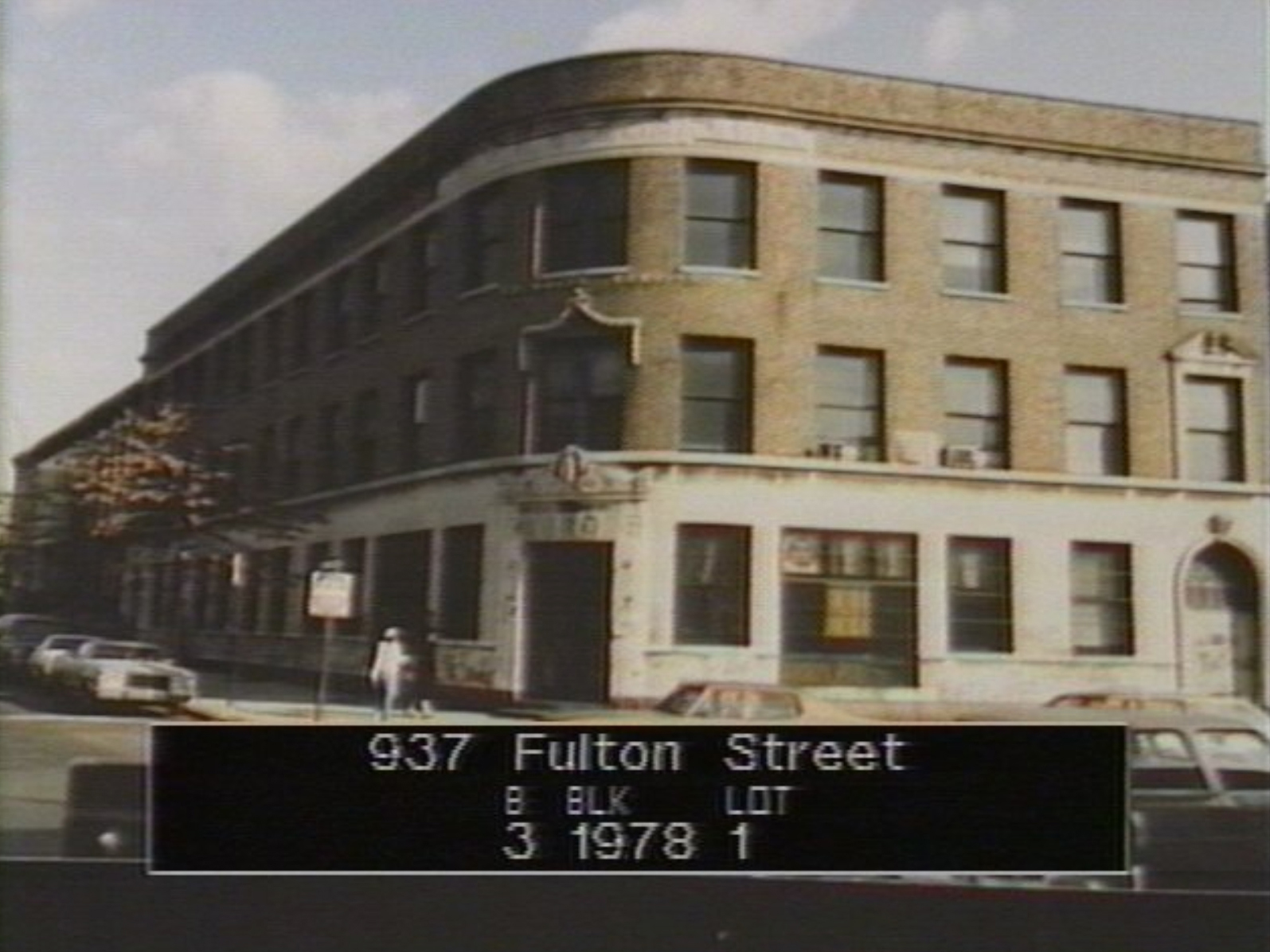
The Addiction Research and Treatment Corporation (ARTC), established in 1969, was one of New York City’s first methadone clinics. Located in a four-story, prewar building on the corner of Fulton Street and Waverly Avenue — in the former headquarters of the Jewish, immigrant-owned Rubel Coal and Ice Corporation — the clinic straddled the borders of the predominantly Black neighborhood of Bedford-Stuyvesant and newly gentrifying Fort Greene, which by the 1970s, was “rapidly becoming blocks of middle-class ‘haves’ and . . . blocks of Black and Brown ‘have nots.’”[5] According to Dr. Beny J. Primm — a Black anesthesiologist and former director of narcotics control at Harlem Hospital who became the ARTC’s medical director — the clinic was “aimed at the hard-core addict in the urban ghetto” and was “run by and for Blacks.”[6] By 1972, the ARTC served a total of 1,300 patients, most of whom were Black. Alongside methadone, the clinic offered a comprehensive approach to treatment, including counseling and employment services. Contrary to federal law, Primm refused to regularly monitor his patients’ urine for other substances and would not “dismiss” a patient if their urine came back positive for something other than methadone. He also used lower doses of methadone than what was recommended in the scientific literature.
It didn’t take long for the ARTC to start attracting critics. In the early 1970s, members of the Fort Greene Crisis Committee (FGCC), a group composed predominantly of white property owners, waged a years-long battle to oust the ARTC from the neighborhood. In 1973, William Graburn, a finance executive and the head of the FGCC, penned a fiery letter to the editor in The New York Times, claiming that ARTC patients “[intimidated] local residents” and that most of these patients were not from Fort Greene, but from Bedford-Stuyvesant. To FGCC members, the ARTC — with its predominantly Black patient population, staff, physicians, and nontraditional approach to methadone treatment — was turning Fort Greene into a ghetto. From the early to mid 1970s, the FGCC would work in concert with federal methadone program auditors and city politicians to surveil, police, and ultimately threaten to freeze the funds of the ARTC.
The FGCC wanted the ARTC to disappear from Fort Greene, so the neighborhood group used their money and political power to chip away at it. Graburn and his supporters pressured the ARTC to open satellite locations in Bushwick and Brownsville, both predominantly Black neighborhoods, that would each treat “an additional 200 addicts” to decrease the presence of people on methadone who were being “dump[ed]” into Fort Greene. Even local politicians used the ARTC as bait. Congressman Fred Richmond, a white Democrat who represented areas of downtown Brooklyn and Fort Greene, used the ARTC as a political wedge to cater to his growing white voting base. Richmond threatened to shut down the clinic if a federal audit of the ARTC — which would expose the clinic’s decision not to comply with federal laws like routine urine screens, among other indictable offenses — was not made public. A New York Amsterdam News reporter stated that “Richmond’s efforts at destruction are not directed at the drug traffic, but at a rehabilitation program that is struggling against massive odds to aid his [Richmond’s] Black constituency, and at a Black physician [Primm] who has spent the last fifteen years of his life working in the service of the poor and oppressed.”[7]
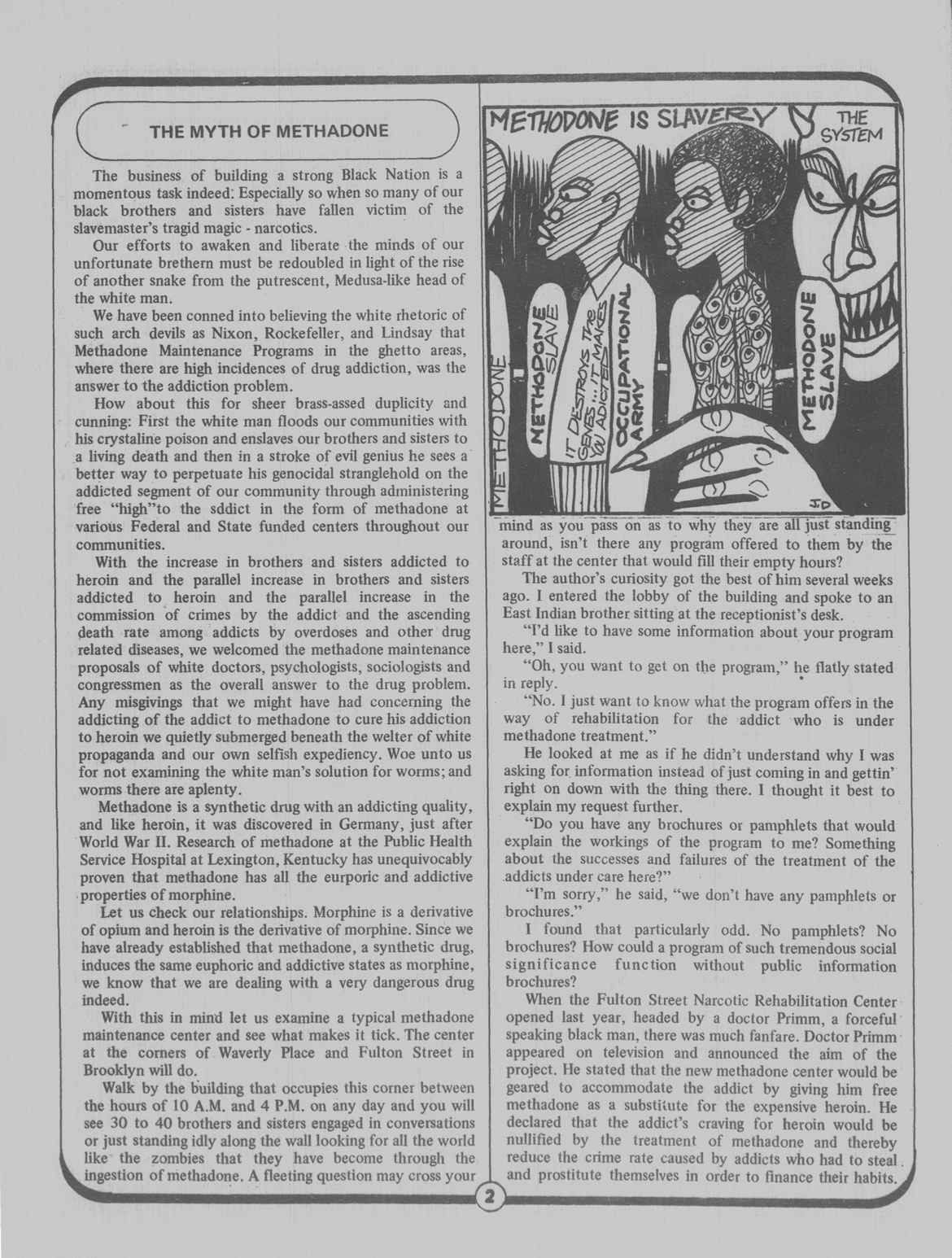
Growing impatient that the federal audit and city-level investigations were taking years to complete, members of the FGCC took matters into their own hands. Frances Mitchell, a white female Fort Greene community planning board and FGCC member, visited the ARTC and demanded to look through patient files to make sure that patients lived in Fort Greene. New York Amsterdam News also reported that another “FGCC sympathizer” had “smuggled . . . sensitive information” pertaining to the ARTC out of the City Comptroller’s office. And it wasn’t just white gentrifiers who came after the ARTC. Black Power activists targeted Primm and the ARTC shortly after its founding. In a 1970 Black News article, an anonymous author labeled the ARTC as “one more of white Amerikkka’s experiments in genocide against black people.”[8] The author argued that Primm, in promoting the ARTC to “much fanfare,” had aligned himself with the “white doctors, psychologists, sociologists and congressmen” who perpetuated the continued enslavement of Black communities through methadone.
According to a June 1970 New York Times article, about a year after the ARTC opened its doors, Primm hired current and former Marine Corps members carrying nightsticks to act as clinic guards after he received threats of violence from “black militants” who might “invade the center.” Primm also made the decision to hire guards after “antimethadone militants” had physically attacked the ARTC’s administrative director in the parking lot outside the clinic. Federal and city employees, local politicians, white gentrifiers, and Black activists all fiercely organized against the ARTC to further their distinct political agendas. The consistent threat and reality of violence towards the ARTC and their staff illustrates just how intense people’s feelings were toward this novel treatment. While intended to be a medical space for the treatment of addiction, the ARTC became a militarized zone of conflict subject to varying degrees of local and federal scrutiny. Methadone was a potent and threatening political symbol of racism, social control, community corruption, and deviance that eclipsed its novel use as a treatment for heroin addiction.
Despite community pushback, the ARTC — renamed START Treatment and Recovery in 2013 — still operates and dispenses methadone at 937 Fulton Street. Since 2008, residents in Fort Greene have tried to shut down, “consolidate,” “downsize,” and more heavily police the location, referring to the area surrounding the clinic as a “drug bazaar.” Much like Harlem, 937 Fulton Street is in an area of Brooklyn that is oversaturated with methadone clinics.
The ARTC is just one example in a broader narrative of rising community tensions surrounding methadone during the early and rapid expansion of MMT programs in New York City. During the early 1970s, methadone programs rarely stayed put. They were fragmented into multi-site clinics, placed in temporary or makeshift locations, or shut down altogether. In June of 1971, a MMT program took over the Gold Star Mother, a retired Staten Island ferryboat that had been laid to rest in Battery Park City on Manhattan’s West Side. Federal government crackdown — rather than community protests — explained this clinic’s relocation. According to the Justice Department’s Bureau of Narcotics and Dangerous Drugs, the West Side Medical Centers, a network of private MMT programs located on the Upper West Side of Manhattan, were dispensing methadone “indiscriminately.” Patients were “poorly screened and inadequately monitored.” After the West Side Medical Centers closed, patients had to receive their doses “at what used to be the refreshment stand.” Until patients were accepted at other programs across the city, a floating clinic would have to suffice.
Patients panicked when they heard of these clinic closures and relocations and were often “left stranded” until they were assigned to an alternate clinic. One 23 year-old patient who was impacted by a private MMT program closure and would be treated “temporarily” on the Gold Star Mother stated, “If I have to wait I’ll be back shooting drugs. I waited three years to get on the city program and didn’t make it.” A Times reporter characterized the Gold Star Mother in carceral terms, calling it a “holding unit” for people who had been displaced from other treatment programs. In a desperate act to save doses, Dr. Robert Newman, the physician in charge of the MMT program roll-out in New York City from 1970 to 1974, used his one-year-old son’s stroller to shepherd leftover methadone bottles from the West Side Medical Centers to the Gold Star Mother.
Meanwhile, in the summer of 1971, Long Island College Hospital in Brooklyn received funding from the city to establish a methadone clinic in the basement of St. Augustine’s Preparatory School, a parochial school on 165 Conover Street in Red Hook. The Red Hook building was a haven for its 550 students: a fire had destroyed the original St. Augustine’s School, located in Bedford-Stuyvesant, about two years prior. On Monday, October 4, a non-violent protest — backed by the school’s principal, a Black reverend named Hanson Jacobs — erupted once parents found out that a methadone clinic would be opening underneath their children’s school. While most parents agreed that methadone could help people, parents didn’t want their children to be “exposed to drug addicts.” About 300 parents stood “shoulder-to-shoulder in the door of the clinic’s prepared quarters,” blocking the clinic’s staff from entering. A community group who supported the clinic assembled in front of the school, forming a modest counter-picket. Patients planning to receive their methadone in the basement of St. Augustine’s that day were diverted to the Red Hook Neighborhood Health Center on 385 Hicks Street. Some got lost in the shuffle and didn’t receive their doses that day, confused upon arrival at the school. The clinic’s staff tried to “persuade the parents to clear the way,” but they failed, and the clinic never opened.
City officials and executive directors of MMT programs, scrambling to redirect methadone provision to thousands of people, used locations like the Gold Star Mother and the Red Hook school basement as tenuous solutions to the closing of private clinics that failed to meet federal criteria or community opposition that ousted clinics from their original locations. According to Dr. Newman (the same physician who used his child’s stroller to transport methadone to the Gold Star Mother), by 1975, it was nearly impossible to open a new MMT program in New York City.[9] For Newman, community opposition to MMT programs revolved around “race,” “class,” “fear,” and “resentment” towards people who used drugs, which generated “hostility” that was difficult for many residents to express before the expansion of MMT programs in the early 1970s.
Methadone clinics allowed community members to redirect their racism, prejudice, and stigma from concepts and people toward physical space. MMT programs could be moved, closed, or abolished, and in talking about “criminals” and “safety,” race and the presumed character traits of “addicts” could be talked around but not necessarily named explicitly. Newman commented: “It was a building, in front of which you could picket, or wheel your baby carriages, or go to the press about . . . people really wanted to express their hostility towards a problem that was so evanescent that they couldn’t do it any other way.”
Above, look through The Methadone Manifesto, via the Urban Survivors Union.
When I asked Syderia how she would feel if the methadone clinic system were to cease to exist, she replied with an answer that almost seemed to surprise herself: “Well, actually, that’s pretty much how I do feel. I think that [patients] should be able to go to the doctor’s office like anybody else and get their meds.” In Canada, Australia, Thailand, and some European countries, primary care providers and pharmacists can prescribe methadone to patients who can pick it up at a pharmacy. No public lines, no observed dosing, no cameras, no guards, no spaces.
Addiction providers, drug policy advocates, and patients on methadone have been calling for more relaxed dosing guidelines for decades with little success. In their “Methadone Manifesto,” patients on methadone who are members of the Methadone Advocacy Group of the Urban Survivors Union have characterized the clinic system as a “deadly culture of cruelty.” The stigma, shame, and logistical obstacles that patients on methadone must navigate on a day-to-day basis has not changed since the 1970s and community organizing against these clinics has not died down. The hurdles required to enroll in a methadone program — even more daunting for those who have a disability, are unhoused, or don’t have reliable access to transportation — prevent people from accessing a lifesaving medication. Methadone clinics continue to disproportionately exist in communities of color and the spaces meant to serve patients are not meant to be seen. The current regime of methadone treatment in this country continues to privilege a system of punishment and suspicion over patient care.
In June 2021, the Drug Enforcement Administration lifted its moratorium on mobile methadone vans, which would help bring methadone to rural areas and underserved communities. While this legislative change seems like progress, it’s reminiscent of the Staten Island ferryboat or the Red Hook school basement. Vans, like ferryboats, are mobile: they can be parked, shut down, and are easier to hide from view. Instead, we need permanence and autonomy for patients on methadone, not another temporary fix. If the spaces — the unmarked facades, the blocks with public lines and police, the basements — remain the same, stigma towards methadone use will persist. If the methadone clinic model were abolished altogether, people living with a chronic disease, like anyone else, could receive their medication at a CVS or Walgreens. Perhaps, then, patients would achieve some form of liberation: from surveillance, from the dehumanizing choreography of swallowing a dose, from damaging myths about their disease and who they are as people, and from the spaces themselves.
The author would like to thank Joanne Meyerowitz, PhD, Professor of History and American Studies, Yale University and John Harley Warner, PhD, Professor of History of Science and Medicine, Yale School of Medicine, for their mentorship while conducting research on this topic, as well as Asher Levinthal, Dr. Kenneth Morford, and Hannah Srajer for their comments on the piece.
Helena Hansen and Samuel K. Roberts, “Two Tiers of Biomedicalization: Methadone, Buprenorphine, and the Racial Politics of Addiction Treatment,” Critical Perspectives on Addiction (2012): 79-102, 91.
Jerome H. Jaffe and Charles O’Keeffe, “From morphine clinics to buprenorphine: regulating opioid agonist treatment of addiction in the United States,” Drug and Alcohol Dependence 70 (2003): S3-S11, S4.
Vincent P. Dole and Marie Nyswander, “A medical treatment for diacetylmorphine (heroin) addiction: A clinical trial with methadone hydrochloride,” Journal of the American Medical Association 193, no. 8 (1965): 646-650.
Mical Raz, “Treating Addiction or Reducing Crime? Methadone Maintenance and Drug Policy Under the Nixon Administration,” The Journal of Policy History 29, no. 1 (2017): 58-86
“Richmond and Pinkett vow fight for ARTC patients,” New York Amsterdam News, Aug 13, 1975, B2.
Beny J. Primm, “Methadone no answer for addiction problem,” New York Amsterdam News, June 24, 1972, A5.
Andy Cooper, “One man’s opinion: Brooklyn political scene,” New York Amsterdam News, June 25, 1975, B1.
“The Myth of Methadone,” Black News 27, no. 26 (1970), 2.
David Courtwright, Herman Joseph, and Don Des Jarlais, Addicts Who Survived: An Oral History of Narcotic Use in America 1923-1965 (Knoxville, University of Tennessee Press, 1989), 346.
The views expressed here are those of the authors only and do not reflect the position of The Architectural League of New York.






Comments