We are celebrating 15 years — and counting — of stories that are deeply researched and deeply felt, that build a historical record of what the city has been.
We are celebrating 15 years — and counting — of stories that are deeply researched and deeply felt, that build a historical record of what the city has been.
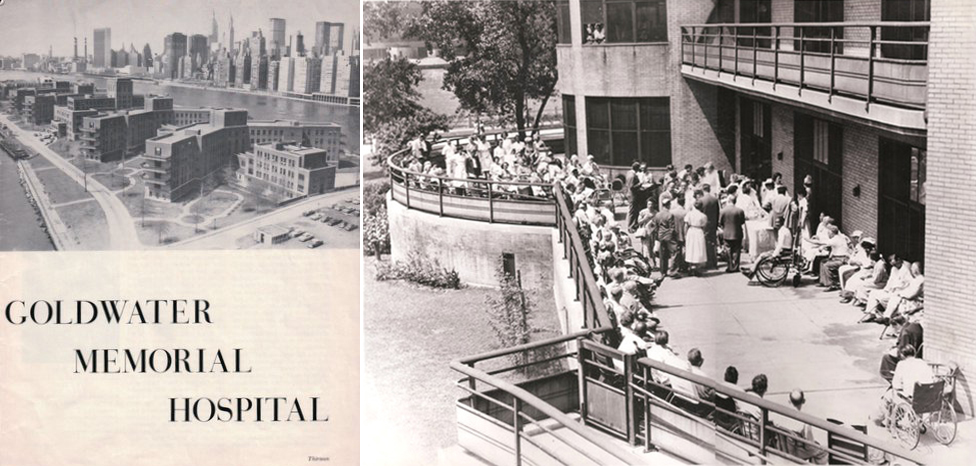
Roosevelt Island, a two-mile sliver of land in the East River nestled between the Upper East Side and Astoria, is home to a population of 12,000 on 147 acres of land. But the island’s small size belies its importance to the history of the city. In its different lives — the land was known as Welfare Island from 1921–1973, and Blackwell’s Island, Hog Island, and Minnehanonck before that — the island has been an influential site of innovations in architecture, medicine, infrastructure, and social service delivery. One such notable institution is the Goldwater Memorial Hospital, known as The Welfare Hospital for Chronic Disease when it first opened in 1939 (its sister hospital, the Bird S. Coler Hospital, opened on the north end of the island in 1952). The immense facility was designed to be a new model of medical care for those with chronic illness. The architect, Isadore Rosenfield, was as concerned with the careful design of a patient’s bedside lamp as he was with the circulation patterns of the thousands of people who would use the facility each day. Rosenfield wrote of the project for Modern Hospital in 1937 that his design was “the first tangible result of agitation, research and educational work over a period of years by…the committee on chronic illness of the Welfare Council in New York City,” and was best understood through an explanation of “the principles in accordance with which it was developed.”
Goldwater closed its doors on December 31, 2013, transferring its patients to other facilities around the city. Today, the buildings are in the midst of being torn down to make way for what the City hopes will be the next chapter in Roosevelt Island’s legacy of innovation: the forthcoming campus of Cornell NYC Tech. A two-million-square-foot applied sciences and engineering campus is planned for 12 acres on the southern half of the island, as part of an initiative launched by Mayor Bloomberg to make New York City a “global leader in technological innovation.”
Photographer and architect Charles Giraudet has been furiously documenting Goldwater Hospital in its last days, compiling an extraordinary 15,000 images so far during the brief window between its de-commissioning and its imminent demolition. Below, Giraudet shares a selection of his photographs (click on any of the photographs below to launch a slideshow with more images) and describes how this archival project has expanded to become, in his own words, “a study of the architect’s intention, of the life and activities in the building, and of light.” –V.S.
The first stone of Welfare Hospital, subsequently renamed Coler-Goldwater, was laid on Roosevelt Island in 1937. Fiorello La Guardia was then mayor of New York and Dr. Sigismund Schultz Goldwater was Commissioner of the Department of Hospitals. Together they planned the development of Roosevelt Island as a haven for medical care and research with the creation of several major pieces of infrastructure, the flagship of which would be Welfare Hospital, dedicated to chronic diseases.
Dr. Goldwater hired a young architect to head the design team. Having emigrated from Russia as a young child and worked as a butcher’s assistant before he went to Harvard to get a degree in architecture, Isadore Rosenfield was to become the Chief Architect of the Department of Public Works. After the war, he would be in charge of New York City’s $100 million hospital program. He wrote several books and articles about hospital design. In a 1937 piece titled “The Fruit of Research“,[1] he describes the scientific process that informed the design decisions at Welfare Hospital. All major programming decisions — from the number of beds to the general layout of the buildings, the angled wings of the wards and the relative heights — were related to an unwavering patient-centric design approach. Going further, the bed itself, with its lighting and relationship to the other beds in the ward, were designed from the ground up to serve two purposes, seen as one: the well-being of the patient and the ability for the doctor to care for him or her.
Roosevelt Island provided Rosenfield with a perfect site. The old penitentiary at the south of the 59th Street Bridge would be demolished so the hospital could take its place. In this low-density setting, patients would benefit from the sun and air necessary to their recovery, while remaining close to their families, an aspect of care that Rosenfield deemed essential.
Away from the constraints of an urban setting, the hospital’s master plan could also yield to its program and develop organically. Four chevron-shaped ward buildings running east-west, connected by a three-story gallery running the length of the site; between the wards’ buildings, two pavilion buildings to receive the families; at the north end, a smaller building housing research laboratories; finally, a central building for admissions, administration, surgery, dorms for visiting doctors and nurses, therapies, and food preparation. All support and technical services were placed in the basement of the various buildings, and a tunnel — running the length of the island — would bring hot water and steam to the facility from a centralized plant that still functions today. Encompassing the width of the island edge to edge, the hospital resembles the superstructure of a ship, the bedrock of Roosevelt Island its hull.
I discovered Goldwater by accident a couple of decades ago, as a young architect from France interested in the nooks and crannies of New York. I was immediately drawn to its angled wings and running balconies reminiscent of the ocean liner architecture of early modernists. There aren’t so many buildings of that era in the country. I grew up near Paris, in a town where, in the 1930s, architects Lods and Beaudoin, associated with Jean Prouvé, built the Ecole du Plein-Air where kids with tuberculosis or other respiratory ailments could be schooled, and I was familiar with Alvar Aalto’s Paimio sanatorium. Goldwater seemed to echo these buildings. They spoke of an age where architecture could ambitiously address social needs for the public good.
Before penicillin, sunlight was part of the cure as much as any medication, so an almost obsessive attention was paid by Rosenfield to the path of light through his buildings. The buildings were placed so that they wouldn’t cast shadows on one another. The chevron shape yielded more hours of exposure and views of the river. Wards were designed to encourage the use of the outdoor space with every bedroom opening onto a wide balcony or terrace. Even the roofs of the main gallery were meant to be used as circulation and terraces by the patients during the sunny months. In fact, almost every single space in the facility receives natural daylight. Corridors set deep in the building are lined by glass partitions or doors with transoms. The dumbwaiter lobby in the laboratory building gets its light from a window set high above the sink of a bathroom that has its own six-foot-high window to the outside. There are countless examples and variations.
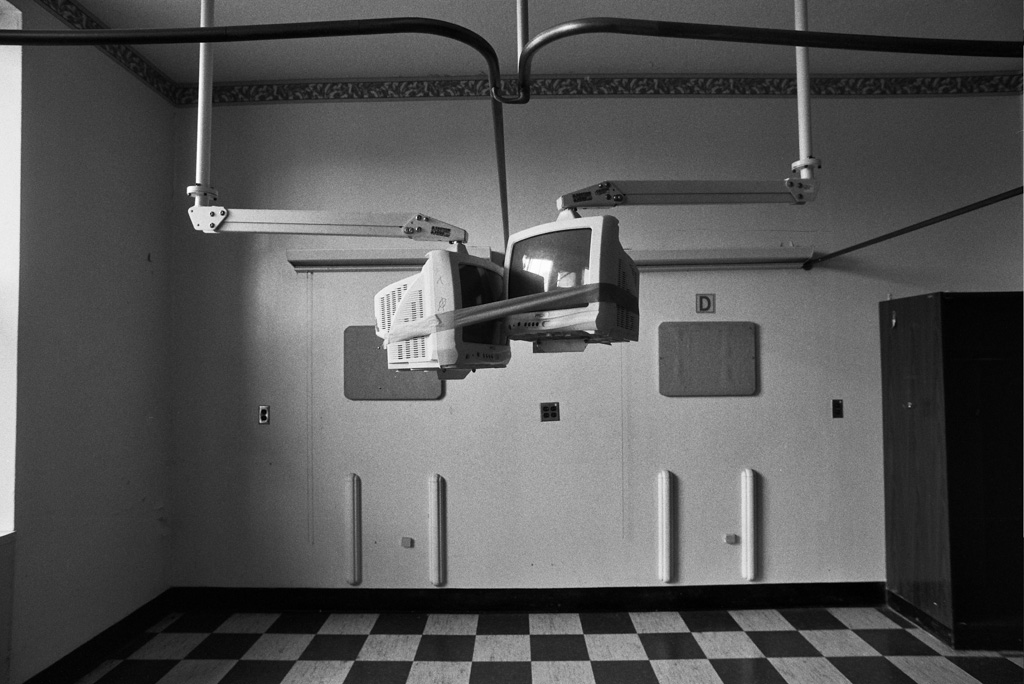
I entered the building during a very special and short phase of its life, between the day when patients and staff had been relocated and rooms had been emptied out of all things not attached to the walls or ceilings and the day the demolition crews would start to tear it down. For the first two weeks, I walked alone in the deserted hallways and basements with my cameras, pushing open doors to rooms that would invariably surprise me. The photo project evolved from a documentation of the “significant spaces” to an encyclopedic project, now totaling 15,000 images. This was due in part to the evolving time parameters of the project and in part to the impossibility of finding any space insignificant in a building so carefully tailored to its use. Ultimately, my photographs became a study of the architect’s intention, of the life and activities in the building, and of light.
Every time period has its light. It is the blank page onto which architect and designers write their projects. Yet, because we view it as part of nature, we have developed little vocabulary to discuss it. Its intensity, temperature, its use in architecture are measured or discussed, but we should consider it a part of culture that is reflected in all its aspects. When it comes to architecture, light is the very substance of space, a cultural trait par excellence. Anyone who walks around or lives in a building of a different era has the experience of a difference in the light’s quality. Movie directors use this to move us through time and space, as it speaks to us through our bodies before our consciousness can awaken to the trick. In a marvelous little book called In Praise of Shadows, Jun’ichiro Tanizaki talks about the influence of western aesthetics on a Japanese man. The western taste for light, brightness, clarity, brilliance, total transparency, and sheen is compared with the soothing, soul-feeding qualities of the deep shade, the murkiness of texture, the patina of time.
What Tanizaki describes is the tactility of light, what our bodies are able to register of the texture of a surface without touching it, how a surface changes depending on how it’s lit — hard to soft, superficial to deep, slick to rutted — how our bodies would feel if immersed in that surface, and how that surface is merely a threshold to the surrounding space. Through our senses, light and touch are connected and always entertain a relationship, of affinity or dissonance, whether or not we’re aware of it. We touch what we see before we touch it and it may even be that some of us can’t see what we can’t touch[2]. In the darkness one can better feel the density of space, often experienced as claustrophobia in our day and age where luminosity is brought everywhere. We have lost the ability to move in darkness comfortably like we have lost the taste for feeding from silence.
Moving through the deserted hospital, enveloped in darkness, or basking in the sunlight drenching the day rooms in the evenings, I came to realize that a different sensibility and aesthetics from ours had informed the design, coming from a time of less disregard for the body’s comfort and functions. Goldwater is superbly built and entirely lined with green and honey-glazed bricks that deepen in tone with incandescent lighting. Its 2700 windows are made of bronze and work like they did on day one even after years of being screwed shut. Until renovations introduced a measure of vinyl and plastic, your hand would touch only wooden handrails and doors, brass knobs, marble windowsills. We have so distanced ourselves from the aesthetics of the ‘30s and the values that informed them that we often associate natural materials and their aging with grime. The gentleness with which light touches these surfaces and the sensation that remains can be so unsettling to the modern hand — the hand that expects the antiseptic and inorganic qualities of whiteness — that it’s easy to forget that the facility merely required a good cleaning on the outside, an operation that fell low on the priority list due to a chronic lack of funding for maintenance (the building is spotless inside).
Goldwater first served as a chronic diseases research facility. During World War II conscientious objectors volunteered to be used as guinea pigs for secret experiments on malaria and extreme cold. Tylenol was partially developed there. Eventually, the south side became a nursing home while the north side evolved into a respiratory care, hospital and rehab facility. In 1970 a new building opened at the south end, designed by William Lescaze, housing chapels for four religions, a library, a radio station, a gym, and a large sports arena and auditorium with a full sound and light stage. Research was abandoned and the laboratory building was used for nurses’ training and administration. Meals were no longer prepared from fresh ingredients and the operating rooms became doctors’ offices. Over the years, the facility had to adapt to changing safety requirements that condemned the balconies and limited the window openings to six inches, along with other, often nonsensical, alterations. The forest was lost for the trees. These mandated changes forced hundreds of air conditioners onto the facades like so many pimples, closed access to the galleries’ roofs, choked the circulation. Parking lots replaced the landscaping on the east side. But because Goldwater was home to people living and working there around the clock who cared for it, it remained a vibrant place and retained its humanity and dignity even when it was stripped of its purpose and its occupants.
There is much to be learned from the study of Goldwater. A number of its qualities are precisely what we are trying to re-instill in many contemporary buildings, including in our tech-centric – as opposed to patient-centric — hospitals where almost anyone will become dazed and confused after a short stay. Air, sunlight, natural materials, attention to circadian rhythms, access to the outdoors, generous space that adapts to a body’s movement rather than requiring that adaptation from the user can’t be considered replaceable by technological prosthetics without consequences for the people and activities for which the building is designed in the first place. Architecture should be about sheltering human activities, not processing them.
There is also something to be learned about the relationship between urban design and architecture: Rosenfield thought he was building a facility, but Goldwater was a de facto small city. At the core of his design were urban principles setting relationships between the buildings themselves and the site, expressing the relationship between the new community and New York as a whole. The hospital was part of a much larger project to build not just the infrastructure of New York, but also its community. The urban realm manifests a culture’s identity and values; it reflects its soul. Only too often nowadays does architecture try to manage what urbanism should, resulting in hyper-expressive buildings reflecting the fascination with the formal exploration unleashed by new CAD tools rather than an interest for the satisfaction of social needs.
But Goldwater is also a lesson in what we can expect of an enlightened city administration whose vision is focused on the welfare of its constituents, and of architecture when it seeks modestly but ambitiously to embody these values. As the hospital enters its final hours, we can ponder the loss of yet another public health facility at a time of intense privatization of the sector and decreasing access to quality healthcare and eldercare for so many. We can use the example of Goldwater to reflect on the way healthcare is currently being delivered to New Yorkers and what has been lost since 1938, when Rosenfield conceived of the architectural experience as a path to well-being for all New Yorkers.
The author would like to acknowledge Judy Berdy, President of the Roosevelt Island Historical Society, who provided most of the historical background used in this article and generously shared her deep knowledge of Goldwater, its history and the people who lived and worked there; Andrew Mongiardo, Goldwater’s former Facility Director, who spent 37 years maintaining the building and came time and again to the hospital after work hours to graciously answer all my questions; and Andrew Winters, Director of Capital Projects and Planning for Cornell Tech, for granting me access to Goldwater.
Unless otherwise noted, all images © Charles Giraudet, All Rights Reserved.
Isadore Rosenfield, The Fruit of Research [Welfare Hospital on Welfare Island, New York City], Modern Hospital, 1937 Mar., v. 48, p. 58-64.
Oliver Sacks, To See and Not See in An Anthropologist on Mars (Alfred A. Knopf, 1995).
The views expressed here are those of the authors only and do not reflect the position of The Architectural League of New York.












Comments